KEY POINTS
Most cardiac arrests in the community setting occur as a result of coronary artery disease and cardiac ischemia.
Given the high mortality of cardiac arrest, prevention is crucial.
Cardiopulmonary resuscitation and rapid defibrillation are the keys to successful resuscitation from cardiac arrest.
Advanced Cardiopulmonary Life Support (ACLS) guidelines provide treatment algorithms for the different cardiac rhythms of arrest.
Automatic external defibrillators provide a means for rapid defibrillation by the public.
High-quality CPR and prompt defibrillation when appropriate are the only proven therapies to increase survival from cardiac arrest.
Rapid response teams have been developed to help decrease the incidence of in-hospital cardiac arrest.
Cardiac arrest, defined as the sudden complete loss of cardiac output and therefore blood pressure, is the leading cause of death in the United States and much of the developed world, claiming at least 300,000 lives each year in the United States alone.1 In the majority of cases, myocardial ischemia in the setting of coronary artery disease represents the underlying etiology of arrest. Conversely, cardiac arrest is the initial presentation of myocardial ischemia in approximately 20% of patients.2 A wide variety of other processes can lead to cardiac arrest, including septic shock, electrolyte abnormalities, hypothermia, pulmonary embolism, and massive trauma (Table 25-1).
Etiologies of Cardiac Arrest
| Myocardial ischemia/infarction |
| Primary cardiac arrhythmia |
| Hypothermia |
| Septic shock |
| Trauma |
| Systemic inflammatory response syndrome |
| Tension pneumothorax |
| Myocardial pump failure |
| Pulmonary embolism |
| Cardiac tamponade |
| Ventricular wall rupture |
| Severe valvular disease |
| Infiltrative cardiomyopathy |
| Inflammatory cardiomyopathy |
| Massive hemorrhage |
| Postoperative |
| Trauma |
| Gastrointestinal bleeding |
| Hypoxemia/respiratory failure |
| Pneumonia |
| Pulmonary embolism |
| Status asthmaticus |
| Suffocation, eg, foreign-body aspiration |
| Electrolyte derangement |
| Hyperkalemia |
| Hypocalcemia |
| Drug toxicity/overdose |
| Digoxin |
| β-Blockers |
| Calcium channel blockers |
| Tricyclic antidepressants |
Survival from cardiac arrest remains dismal, even after the introduction of electrical defibrillation and cardiopulmonary resuscitation (CPR) over 50 years ago. In the best cases (witnessed ventricular fibrillation arrest with rapid defibrillation), survival to hospital discharge ranges from 30% to 46%,3,4 although overall out-of-hospital arrest survival is usually much lower, ranging from 2% to 26%.5 In large American cities, out-of-hospital arrest survival may be even worse—survival rates of 1.4% and 1.8% have been reported for New York and Chicago, respectively.6-8 Even after successful resuscitation from cardiac arrest, most patients die within 24 to 48 hours despite aggressive intensive care treatment. Reperfusion injury, a subject of much basic science investigation, is thought to be involved in this postarrest deterioration.9,10
Demographic data from multiple studies demonstrate that the mean age of patients who suffer out-of-hospital cardiac arrest is approximately 68 to 70 years, with a slightly higher incidence in men than in women.1,2,11 Over 70% of these patients experience arrest in the home or other residential location.12,13 In-hospital cardiac arrest patients exhibit similar demographics, with one survey showing a mean age of 71 years and also somewhat higher incidence in males.14 There do not appear to be significant survival differences between men and women.2
To standardize treatment during cardiac arrest, a number of treatment algorithms have been developed based on laboratory and clinical evidence. These have been compiled into the Basic Life Support (BLS) and Advanced Cardiopulmonary Life Support (ACLS) guidelines published and updated regularly by the American Heart Association’s Emergency Cardiac Care Committee,15 as well as other international resuscitation organizations (International Liaison Committee on Resuscitation).15 For additional information about ACLS guidelines and their revisions, see the contact information listed in Table 25-2.
Contact Information for BLS and ACLS Training and Resources
| American Heart Association (AHA) |
| Web site: www.heart.org |
| Telephone: (800) 242-8721 |
| American Red Cross (ARC) |
| Web site: www.redcross.org |
| Telephone: (800) 733-2767 |
| European Resuscitation Council (ERC) |
| Web site: www.erc.edu |
| Telephone: +32 3 826 9321 |
PEDIATRIC CARDIAC ARREST
The majority of discussion in this chapter pertains to adult cardiac arrest because cardiac arrest in children, fortunately, is much less common. When it occurs, pediatric cardiac arrest more often is secondary to trauma or pulmonary derangements, such as drowning, status asthmaticus, or foreign-body obstruction, rather than due to a primary cardiac arrhythmia.16 However, ventricular fibrillation does occur in the pediatric population.17 Guidelines for pediatric resuscitation have been established and are compiled in the Pediatric Advanced Life Support (PALS) manual. For neonates, in whom cardiac arrest is yet another specialized problem, the manual Neonatal Advanced Life Support (NALS) has been developed. While many of the general principles of this chapter also apply to children, readers should refer to these additional texts for more detailed information.15
PREVENTION OF CARDIAC ARREST
Given the poor prognosis of cardiac arrest, prevention remains the best hope to save lives. To this end, out-of-hospital and in-hospital cardiac arrests require different prevention strategies.
In the outpatient setting, careful attention to coronary artery disease risk factors such as smoking, hypertension, and hypercholesterolemia, and aggressive treatment for these conditions can lower the risk of myocardial ischemia and therefore the risk of cardiac arrest. In consultation with their physicians, most patients with multiple cardiac risk factors should be treated with aspirin to lower the probability and severity of myocardial infarction. Patients otherwise at risk for sudden death, such as patients with bouts of ischemic ventricular tachycardia and/or a history of myocardial infarction with subsequently depressed ejection fraction, should be considered for implantable cardioverter defibrillator (ICD) placement (reviewed in refs. 18 and 19). The use of ICD devices remains an area of active investigation and likely will expand as smaller and less expensive devices are developed.
In the in-hospital setting, where sudden ventricular fibrillation/ventricular tachycardia (VF/VT) from coronary events is not the most common mechanism of arrest, prevention requires a different approach. Several studies have demonstrated that hospitalized patients who suffer cardiac arrest frequently exhibit signs and symptoms of destabilization up to 12 hours before they become pulseless.20,21 These symptoms include vital sign changes such as progressive hypotension, tachycardia, hypothermia, or hypoxia. They also include clinical changes such as mental status deterioration or progressive shortness of breath. Therefore, nursing staff should be appropriately vigilant in monitoring for such changes, and physicians should be duly attentive to warning signs from patients and staff. Early stabilization by such measures as intubation, initiation of vasopressor therapy, and/or transfer to an intensive care unit are far more effective than treating cardiac arrest once it has occurred. In an effort to prevent cardiac arrest, rapid response teams have been implemented, which include health care providers who are trained to recognize and treat the early signs of destabilization that may lead to cardiac arrest. This concept was formalized in Europe and Australia and is now being used in the United States with increasing frequency in diverse hospital environments.22-24
RESUSCITATION TEAM ORGANIZATION
It is very important for hospitals, ICUs, and prehospital care systems to establish a clearly delineated team structure for cardiac arrest treatment. In-hospital studies have shown that a well-trained and organized arrest team is an important component in the resuscitation from sudden death.25 Team members should be ACLS trained and have a specified team leader who will lead the resuscitation efforts. Training should emphasize the need for a hierarchical structure, with the team leader making most treatment decisions, to prevent the confusion that often occurs during cardiac arrest events. It also should be emphasized that response time is critical, such that a resuscitation team should be able to arrive on the scene of a cardiac arrest within minutes to initiate treatment. Recent data demonstrate that groups with best-practice survival from cardiac arrest have mean “call to shock” times (for VF/VT arrest) of 5 minutes or less,26 and certainly the earlier the response, the more likely a better outcome will be obtained. Resuscitation efforts during cardiac arrest require activities to be performed quickly, calmly, and in regimented fashion. Rescuer panic and disorganized efforts are counterproductive and can best be avoided by appropriate training before (and debriefing after) events take place. With the growth of medical simulation technology and sophisticated manikins for resuscitation training, it is possible for cardiac arrest teams to rehearse scenarios to supplement education and enhance preparedness.27,28
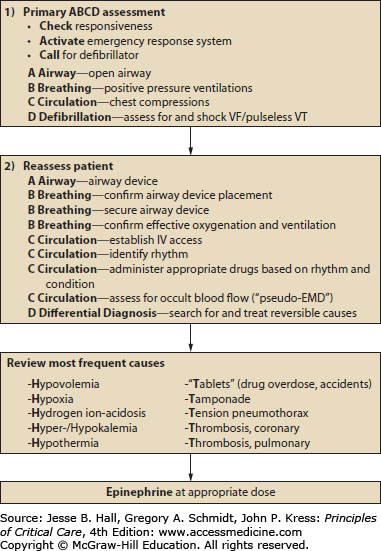
BASIC LIFE SUPPORT
The first steps of resuscitation from cardiac arrest involve what is known as basic life support (BLS). These fundamental skills are part of CPR training courses offered to the public by organizations such as the American Heart Association and the American Red Cross. Given the importance of early recognition and care for cardiac arrest, it is incumbent on all medical personnel from ward receptionists to radiology technicians to physicians to maintain BLS training. Health care workers also should encourage the public to obtain these skills, which are often summarized by the ABCs—airway, breathing, and circulation. With the release of the 2010 international consensus resuscitation guidelines (published in the United States through the American Heart Association), increased emphasis has now been placed on circulating oxygenated blood during out-of-hospital cardiac arrest resuscitation efforts and de-emphasizing airway evaluation and ventilation—now summarized by CAB instead of ABC—circulation, airway, and breathing.15
INITIAL ASSESSMENT
The assessment of “Look, Listen, and Feel” has been removed from guidelines recommendations pertaining to the initial assessment and emphasis has been placed on immediate chest compressions. If a patient is deemed unresponsive, the initial observer should immediately call for help while assessing the patient and providing initial care, following the new format of CAB (see above).
The hemodynamic status of the patient should be assessed via palpation of arterial sites. As an approximate guide, the radial, femoral, and carotid pulses are lost at systolic pressures below 80, 70, and 60 mm Hg, respectively.15 Therefore, the most sensitive site to assess is the carotid artery. If no pulse can be felt at the carotid, chest compressions should be initiated immediately. Compressions should be performed at a rate of at least 100 beats per minute and to a depth of at least 2 in.
Recent studies have demonstrated the importance of “good quality” chest compressions, partially defined by compressions performed at the appropriate rate and depth. This is important in light of the fact that studies have shown performance of chest compressions to be grossly suboptimal and highly variable in actual practice.29-30 Rescuers should pay particular attention to the performance of this skill. Newer generations of monitor/defibrillators, currently available but not widely implemented, may aid this process by monitoring the quality of chest compressions and generating alarms during suboptimal performance. Intriguing recent data have suggested that chest compressions may be more important than defibrillation in the initial treatment of cardiac arrest.31,32 These observations, which might have been considered heretical just several years ago, lend support to an important paradigm in cardiac arrest, that of the three-phase model of cardiac arrest (see discussion later in this chapter).33 Other methods to improve CPR performance have also been shown effective, including performing a series of uninterrupted chest compressions followed by one shock continued with another series of uninterrupted chest compressions.34 This push for continuous chest compressions stresses the need to circulate the oxygenated blood throughout the body during cardiac arrest resuscitation efforts.
Monitoring the adequacy of the circulation during performance of CPR traditionally has been based on palpation of pulses, which is now generally considered to be highly unreliable. Capnography is an attractive adjunct to bedside clinical monitoring because the amount of carbon dioxide returned from peripheral tissues and then exhaled from the lungs should be a measure of the adequacy of cardiac output. In one prospective, observational study,34a 150 consecutive out-of-hospital cardiac arrests were monitored by end-tidal carbon dioxide levels after intubation. After 20 minutes of advanced cardiac life support, end-tidal carbon dioxide levels averaged 4.4 ± 2.9 mm Hg in nonsurvivors and 32.8 ± 7.4 mm Hg in survivors (p < 0.001). A 20-minute end-tidal carbon dioxide value of 10 mm Hg or less successfully discriminated between 115 nonsurvivors and the 35 patients who survived to hospital admission. While not yet routine, capnography may be useful for both judging the adequacy of resuscitative efforts and offering prognostic information. The American Heart Association 2010 Guidelines recommend using capnography during resuscitation.35
While not strictly part of BLS, fluid resuscitation is a crucial adjunct to circulatory support in the initial phases of resuscitation, especially during arrest with pulseless electrical activity as an initial rhythm. Intravenous access should be obtained rapidly if it is not already present, and adult patients should receive a rapid infusion of at least 500 to 1000 mL of 0.9% saline or lactated Ringer’s solution. In children, the crystalloid infusion should be calculated at 20 mL/kg. The ideal IV access would include a peripheral large-bore (ie, 14-18 gauge) catheter, intraosseus line, and/or large-bore central catheter (ie, not a double- or triple-lumen catheter). If a central-line approach is chosen as opposed to a peripheral IV, the optimal site for central-line placement in resuscitation is the femoral vein. Since the chest and neck are active sites for chest compressions and ventilatory support, respectively, subclavian or internal jugular approaches are impractical unless already present.
AIRWAY
To attempt optimal airway opening, the chin should be lifted, and the jaw should be thrust forward. A quick evaluation of the oropharynx should be performed to look for a foreign body, blood, or other occluding material. Any visualized foreign body should be removed by suction or by careful use of fingers or forceps. After this evaluation, several “rescue breaths” should be delivered via mouth-to-mouth or mask-to-mouth technique. If the chest wall does not rise with these breaths, it is possible that a complete airway obstruction exists, and abdominal thrusts should be performed to attempt airway clearance. If these fail, trained personnel may need to establish a surgical airway via cricothyrotomy.
BREATHING
While holding the chin and jaw in the correct position, breaths should be delivered during initial efforts until a more definitive airway can be obtained. In cardiac arrest, this is performed via endotracheal intubation, which is performed routinely by anesthesiologists, emergency physicians, respiratory therapists, and paramedics. If possible, ventilation should be performed with maximal [Math Processing Error] via bag-valve mask until intubation is performed. Pulse oximetry can be used to monitor patient oxygen saturation during this process.
VENTRICULAR TACHYCARDIA WITH A PULSE
Ventricular tachycardia (VT) may or may not generate a pulse. Therefore, it is crucial to assess the hemodynamic status before ACLS resuscitative measures are begun. If the patient has a pulse, is conscious, and has only mild complaints of palpitations, mild chest discomfort, weakness, and/or anxiety, electrical cardioversion can be considered with initial synchronized shocks at 100 J or higher. If the patient exhibits signs of instability, including syncope, severe chest pain, or marked hypotension, then cardioversion should proceed immediately after appropriate sedation is delivered.
The treatment of VT with a pulse includes intravenous administration of amiodarone or lidocaine and supportive care (oxygen administration and preparation for electrical cardioversion). The use of procainamide, amiodarone, sotalol, and/or magnesium can also be considered appropriate for use. Recurrent VT often requires electrophysiologic evaluation and treatment, including the placement of an ICD (reviewed in ref. 35).
VENTRICULAR FIBRILLATION/VENTRICULAR TACHYCARDIA WITHOUT A PULSE
Ventricular fibrillation and ventricular tachycardia without a pulse (VF/VT) are grouped together because both require the same treatment—immediate defibrillation. In fact, defibrillation should precede any other assessment or treatment. Studies have shown consistently that the earlier a patient is defibrillated successfully, the better are the chances for survival.36 This observation has stimulated the use of automatic external defibrillators (AEDs) in airports and other public locations (see the section on AEDs later in this chapter).
When a patient is found in VF/VT, a biphasic defibrillator should be used to provide one rapid shock, with careful attention to minimize pre- and postshock pauses in chest compressions (<5 seconds) (see Fig. 25-1 for a VF/VT algorithm). Chest compressions should be immediately continued for 2 minutes after the shock without interruption. For institutions using standard monophasic defibrillators, the first shock should be delivered at 200 J; the next two shocks can be delivered at 200 J or at 300 and 360 J, respectively per the energy escalation proposed in the ACLS guidelines. Using biphasic defibrillators (see later in this chapter for a discussion of different defibrillator types), all shocks should be delivered at 150 to 200 J or at the energy suggested by the manufacturer.4
FIGURE 25-1
ACLS algorithm for VF/VT. Perhaps the most important aspect of this algorithm is the need for early defibrillation. ACLS algorithm for PEA. Note that this algorithm really serves more as a prompt for differential diagnosis; see Table 25-3 for elaboration of PEA etiologies. (Data from American Heart Association ACLS Manual.)
If a patient remains in pulseless VF/VT immediately after the shock, further treatments include assessment of the CAB’s and pharmacologic adjuncts. Chest compressions should be initiated immediately, with care taken to ensure compression quality, as discussed previously. Patients should be intubated immediately and ventilated with 100% O2, with care taken to ensure correct endotracheal tube placement by both auscultation and end-tidal CO2 detection, if available. Providers should take care not to hyperventilate patients during resuscitation and pay close attention to hyperoxygenation once the patient regains their pulse. A recent study found that patients who had arterial hyperoxia after their cardiac arrest had increased mortality compared with normoxia or hypoxia though this concept is still an area of active research.37
If not already performed, IV access should be established. Large-bore (not multilumen) central venous access by the femoral approach is most convenient and practical in this setting if skilled personnel are available. It is often useful to obtain an arterial blood gas sample at this point as well because it will take some time for the results to return to the team in any case. While these steps are taking place, the arrest team leader should rapidly obtain a very brief history from available sources, including nursing staff, family, or physicians caring for the patient. The most important details to obtain are when the patient was last seen with a pulse, what pertinent medical problems the patient has, and what has taken place in the last few hours of patient observation.
In VF/VT arrest, either epinephrine 1 mg IV or vasopressin 40 U IV should be given early, preferably within the first 3 to 5 minutes of resuscitation efforts. Vasopressin has been shown to improve coronary perfusion pressure and possibly improve initial resuscitation compared with epinephrine.38-39
Related posts:






Full access? Get Clinical Tree


