Figure 9.1
(a) Left breast wire localization prior to lumpectomy. (b) Radioactive seed localization of inferior breast lesion
Surgical Procedure
Anesthesia for a breast surgery can involve the use of local anesthetic with sedation, a paravertebral block or general anesthetic. Incision placement for a surgical biopsy or lumpectomy can vary depending on the size and type of lesion to be excised. For a known benign lesion either an incision directly over the lesion or a periareolar incision which facilitates access to the benign lesion can be selected if cosmesis is of importance to the patient and a periareolar incision will not compromise future breast feeding in premenopausal women. For an excisional biopsy of an unknown abnormality the incision with the most direct access to the area is desired. Mammographic or MRI localization may not have facilitated placement of a localization wire directly adjacent to the lesion so the surgeon must evaluate the location of the abnormality and determine the best incision placement without necessarily following the wire through the breast which may lead to an excess of tissue removed. Incision placements are commonly radial in the lower breast and periareolar or along Langer’s lines in the superior breast but should be selected based on patient breast size, lesion size and best location to avoid a convexity post surgical removal. Excision of a lesion can use electrocautery, knife or scissors depending on surgeon preference. Once removed, the specimen requires orientation in three dimensions, using either suture, clips or ink (Fig. 9.2). Even if known to be benign a breast lesion should be oriented to prevent need for re-excision if an unsuspected cancer is detected. A radiograph of the tissue is then necessary for non-palpable lesions to ensure inclusion of the area of concern. If a biopsy was performed pre-operatively for the diagnosis, then often a metallic clip will be present and should be confirmed within the specimen as well as the lesion of interest. A 3-0 Vicryl suture should then be used, in an interrupted fashion, to re-approximate the deep dermal layer. A 4-0 Monocryl or non absorbable suture (which will be removed post operatively), in a running fashion, should finally be used for the subcuticular layer. Apply either Steri-Strips or a liquid adhesive to the skin to complete the operation.
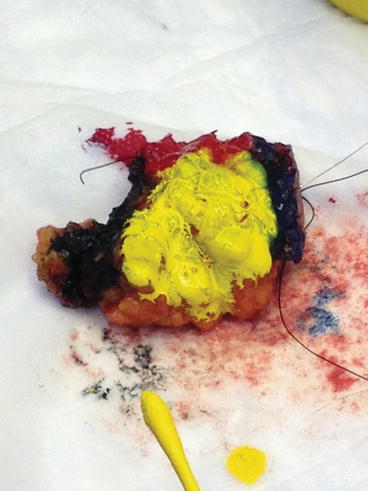
Figure 9.2
Inking of a lumpectomy specimen
Nipple Exploration
For nonlactating patients with bloody nipple discharge or unilateral spontaneous discharge, nipple exploration and duct excision is recommended. The procedure is performed once examination has confirmed the discharge and imaging is negative for abnormality that is amenable to biopsy. The procedure involves use of local or regional anesthesia with incision placement in a periareolar location near the duct with discharge. The patient should be advised to not express the discharge for several days prior to the surgery. The breast tissue is incised up to the posterior ducts and then a lacrimal duct probe placed through the duct of interest. Blunt dissection is performed to the duct and then the duct excised with knife or cautery from the nipple insertion site to 5-7 cm deep into the breast. The lacrimal duct probe is removed once the duct is identified and excision started. The specimen is oriented and then the breast tissue closed with 3-0 Vicryl and skin closed with absorbable or nonabsorbable suture (to be removed 1 week later in clinic). Steri-strips and dressing are then applied.
Partial Mastectomy/Oncoplastic Breast Surgery
For patients undergoing breast conservation surgery for cancer, the localization procedures with wire, seed or ultrasound are similar to those described in Sect. 9.2. The only note of difference is that for patients with several abnormalities (multi-focal disease within one quadrant of the breast) which are felt to be amenable to partial mastectomy several wires may be used for “bracketing” of a lesion. In these and all cases of localization for cancer the surgeon and breast radiologist should discuss the case together to ensure each provider understands the operative plan for the patient. For patients with mulit-centric disease, or cancers in more than 1 quadrant of the breast, currently mastectomy is advised but is undergoing review in a clinical trial to determine if breast conservation is possible for lesions separated by more than 2 cm (Alliance/American College of Surgeons Oncology Group trial Z11102). For multi-focal disease, the operative procedure will likely involve a larger excision than a diagnostic lumpectomy or excision of a benign lesion. Incision placement is frequently over the lesion or periareolar but as more oncoplastic techniques are employed the surgeon may select an incision based on the ability to provide the best internal breast closure post excision [6, 9].
Related posts:







Full access? Get Clinical Tree


