151 Blood Component Therapies
Blood component therapy has had a central role in the development and practice of numerous medical advances, especially in modern surgery. It is only in more recent years that blood transfusion is no longer regarded as essential for a wide range of medical and surgical conditions. It is now possible for most uncomplicated major surgery to be conducted without allogeneic blood component therapy.1 Blood component transfusion is generally supportive therapy for the correction of one or more hematologic deficiencies until the basic disease process can be controlled or corrected. Appropriate attention to accurate diagnosis of the hematopoietic deficiency and consideration of the range of therapeutic options available and their potential hazards are essential before accepting blood component therapy as indicated.2
 Guidelines for Blood Component Therapy
Guidelines for Blood Component Therapy
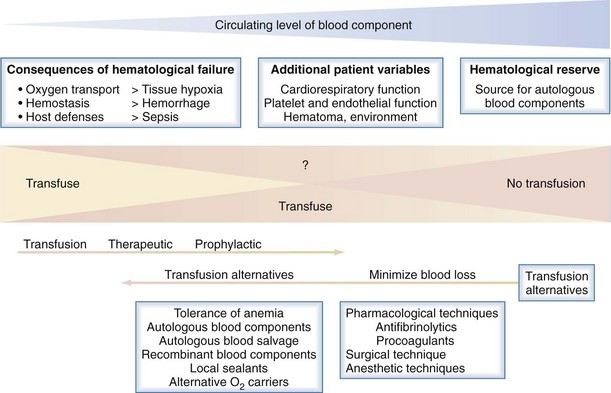
The following is a brief summary of the guidelines for use of commonly available blood components. An evidence-based approach to blood component transfusion has resulted in many long-standing transfusion dogmas being challenged and better guidelines for their use being developed for safe, effective clinical practice. Figure 151-1 illustrates the general approach to the decision to transfuse blood components, with the emphasis on patient blood management and how blood component therapy fits into the bigger picture.1
Red Blood Cell Concentrates
Appropriate and inappropriate use of red blood cell (RBC) transfusions in acute medicine has received considerable attention in recent years; however, identifying the benefits of RBC transfusion in many circumstances has been difficult.2–3 The question of the lowest safe hematocrit continues to receive considerable attention. Pushing any aspect of a system to its limits risks “sailing close to the wind” and may be appropriate in some situations but potentially hazardous in others. In an otherwise stable patient, the transfusion of RBC concentrates is likely to be inappropriate when the hemoglobin level is above 100 g/L. Their use may be appropriate when hemoglobin is in the range 70 to 100 g/L if there are other defects in the oxygen transport system. The decision to transfuse should be supported by the need to relieve clinical signs and symptoms of impaired oxygen transport and to prevent morbidity and mortality, ultimately to improve clinical outcomes. The transfusion of RBC concentrates is likely to be appropriate when hemoglobin is less than 70 g/L and the anemia is not reversible with specific therapy in the short term, but lower levels may be acceptable in patients who are asymptomatic, especially in the younger age group.
Platelet Concentrates
Platelet transfusions may benefit patients with platelet deficiency or dysfunction, and there are some general recommendations for their use.4 Prophylactic transfusion of platelet concentrates is indicated in patients with bone marrow failure when the platelet count is (1) less than 10 × 109/L and there are no associated risk factors for bleeding or (2) less than 20 × 109/L in the presence of additional risk factors. However, recent evidence suggests lower levels may be tolerated if there is no clinical evidence of hemostatic failure.
Fresh Frozen Plasma and Cryoprecipitate
Fresh frozen plasma is widely used, but there are limited specific indications for its use, and there is a dearth of evidence for efficacy in many clinical settings.5–6 The use of fresh frozen plasma may be appropriate in patients with a coagulopathy who are bleeding or at risk for bleeding when a specific therapy or factor concentrates are not appropriate or unavailable. Fresh frozen plasma generally is indicated in hemorrhaging patients for replacement of labile plasma coagulation factors (e.g., massive transfusion, cardiac bypass, liver disease, or acute disseminated intravascular coagulation [DIC]). Fresh frozen plasma is rarely indicated in vitamin K deficiency or reversal of warfarin therapy, because concentrates are now generally available.7 The use of fresh frozen plasma generally is not considered appropriate in cases of hypovolemia, in plasma exchange procedures (unless postexchange invasive procedures are planned), or in treatment of immunodeficiency states.
Plasma-Derived Products
A wide range of highly purified plasma-derived blood products is available for use in numerous clinical conditions. It is beyond the scope of this chapter to discuss their use in detail; Table 151-1 summarizes commonly used fresh and plasma-derived blood products. Fibrinogen concentrate instead of cryoprecipitate is having an increasing role in the management of hypofibrinogenemic states, depending on local availability.
| Blood Product | Main Indications |
|---|---|
| Whole blood* | Rarely indicated in acute hemorrhage if other blood products are unavailable |
| Red blood cell concentrates* | Hemorrhage and anemia |
| Leukocyte-depleted blood* | In patients having febrile reactions, to avoid leukocyte immunization in selected patients (especially patients with hematologic malignancy). Universal prestorage leukodepletion is more widely used and has the added benefit of minimizing storage lesions. |
| Platelet concentrates* | Thrombocytopenia due to marrow hypoplasia or platelet functional defect |
| Granulocyte concentrates* | Occasionally in patients with sepsis associated with profound and prolonged neutropenia secondary to marrow suppression |
| Fresh frozen plasma* | Specific or multiple plasma protein deficiencies (especially coagulation) |
| Cryoprecipitate* | Hypofibrinogenemia and rarely in factor VIII and von Willebrand disease, when concentrates are unavailable |
| 4% or 5% albumin solutions† | Plasma volume expansion. Use is controversial, and the role of albumin solutions in critically ill patients remains under deliberation.30 |
| Concentrated albumin† | Severe hypoalbuminemic states with complicating hypovolemia |
| Concentrate of coagulation factors II, VII, IX, and X† | Vitamin K–dependent factor II, IX, and X deficiency and reversal of oral vitamin K antagonists31 |
| Specific factor concentrates† | Factor VIII and IX concentrates have an established role in management of hemophilia, but others are in the process of establishing their clinical efficacy and indications. |
| Fibrinogen concentrates for hypofibrinogenemia and dysfibrinogenemia32 Antithrombin concentrates are available for thrombophilia due to antithrombin deficiency and are increasingly recommended in other disorders in which antithrombin may be depleted (e.g., DIC, MODS).31 | |
| Gamma globulin† | Generally used intravenously for replacement in hypogammaglobulinemia or in high dosage in autoimmune disorders33 |
| Specific immune gamma globulins† | Rhesus prophylaxis, specific infection prophylaxis (e.g., tetanus, zoster, hepatitis B) |
DIC, disseminated intravascular coagulation; MODS, multiorgan dysfunction syndrome.
Recombinant Blood Products
Development and introduction of recombinant blood components continues to be one of the most exciting advances in transfusion medicine. Recombinant growth factors (cytokines) such as erythropoietin and granulocyte stimulating factors have had a major impact on managing anemia and neutropenia. There are further promising recombinant cytokines in development that could have a role in countless clinical conditions, especially as antiinflammatory and tissue-protecting agents. Recombinant hemostatic factors have improved the management of hemophilia, and recent expansion of clinical indications for the use of recombinant activated factor VII (factor VIIa)—beyond treating hemophiliac patients with coagulation factor inhibitors—is having an impact on management of a range of hemostatic disorders.8 Because factor VIIa is dependent on tissue factor, which is usually available in limited quantities within the circulation, its clinical use is generally regarded safe from a thrombosis-inducing point of view, and its use is now being recommended as a “panhemostatic agent.” Factor VIIa initiates the extrinsic coagulation pathway only when complexed to tissue factor at sites of injury. It may have a role in a wide range of hemostatic disorders (e.g., massive blood transfusion, liver disease, uremia, severe thrombocytopenia, and platelet disorders). It has been difficult to establish a sound evidence base outside the hemophilia setting for the use of rVIIa, with most experience being observational and anecdotal. Randomized controlled trial results have shown a significant reduction in transfusion requirements but could not demonstrate a reduction in mortality. There is also an increased risk of thromboembolism.
 Transfusion Management of Massive Acute Hemorrhage
Transfusion Management of Massive Acute Hemorrhage
Transfusion can be minimized with tolerance of hypotension until hemorrhage is controlled and acceptance of lower hemoglobin levels. The immediate posttransfusion function of stored red cells and hemoglobin in delivering oxygen to microcirculation and in oxygen unloading is also being questioned, with the storage age of RBCs possibly being associated with poorer clinical outcomes.9 Recent animal data point to the immediate clinical benefit of transfused red cells in treating hypovolemic shock relating more to reconstitution of the macrocirculation, with potentially adverse effects on the functional capillary density in the microcirculation.
A protocol approach to blood component therapy has generally not been recommended. However, this remains a controversial issue, with advocates for up-front protocol component therapy with red cell and hemostatic components, especially fresh frozen plasma with or without cryoprecipitate. With better understanding of coagulopathy in the critical hemorrhage setting and the importance of hypofibrinogenemia and hyperfibrinolysis, there is a reanalysis of the approach to blood component therapy. Failure of hemostasis is common in acutely bleeding patients and may be complex and multifactorial. Accumulating evidence supports the view that the pathophysiology of coagulopathy, when occurring in the context of critical hemorrhage, should be viewed as related to the primary insult or initiating event. A secondary coagulopathy may compound the problem in the resuscitated patient, such as massive stored blood transfusion, hemodilution, hypothermia, and continuing tissue hypoxia.10–11 The primary mechanisms of coagulopathy relating to the initiating event may relate to trauma, hypoxia, pregnancy, sepsis, envenomation, or antithrombotic agents.12–13 In all circumstances there is activation or inhibition of some aspect of the hemostatic system, and therapy is better informed if these varied mechanisms are better understood. Frequently, complex tests are required for definitive diagnosis, but the urgency of the situation cannot always wait for the results, and therapy may be initiated on clinical evidence with minimal laboratory information.
Many trauma patients have coagulopathy at presentation related to hypovolemic shock and not consumption or dilution. Recent evidence indicates that activation of the protein C system and hypofibrinogenemia due to secondary hyperfibrinolysis are important.14 Except when severe clotting test abnormalities are present, hemostatic laboratory parameters correlate poorly with clinical evidence of hemostatic failure. In the massively transfused patient, thrombocytopenia and impaired platelet function are the most consistent significant hematologic abnormalities, correction of which may be associated with control of microvascular bleeding. A problem with standard screening tests of coagulation function is they do not provide information about the formation of the hemostatic plug, its size, structure, or stability. Global tests of hemostatic plug formation and stability such as thromboelastography, thrombin generation tests, and clot waveform analysis in which changes in light transmission in routine activated partial thromboplastin time (APTT) are measured are of increasing use. With ongoing bleeding with associated microvascular oozing, various approaches may be taken. Having ensured that all identifiable hemostatic defects have been corrected, questions then arise as to the role of fresh blood and, more recently, recombinant activated factor VII.
 Hazards of Allogeneic Transfusion
Hazards of Allogeneic Transfusion
It cannot be overemphasized that allogeneic blood transfusion is a tissue transplant that is probably associated with the greatest range of potential hazards of any medical intervention and should only be used in circumstances in which there is good evidence that clinical outcomes will be improved.15–16
The pathophysiology of transfusion reactions can be divided broadly into three categories:

Full access? Get Clinical Tree


