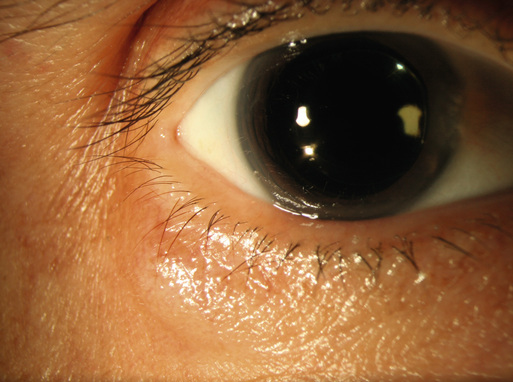
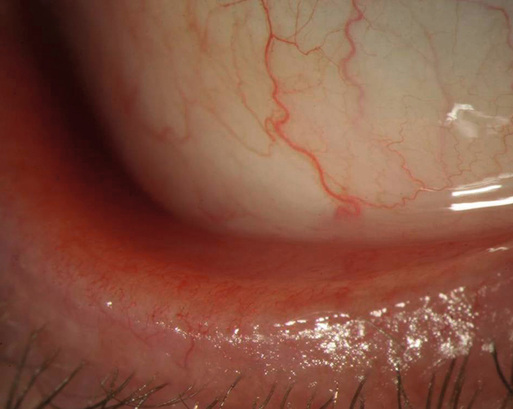
Rebecca Shields, James T. Banta Inflammation of the eyelids, also known as blepharitis, is one of the most frequently encountered ocular diseases. Blepharitis may be of infectious or inflammatory etiology. The disease can be divided into two basic categories anatomically: anterior and posterior blepharitis.1,2 Anterior blepharitis involves the anterior lid margin surrounding the eyelashes and is usually associated with staphylococcal infection or seborrhea. Staphylococcal blepharitis is a disorder that predominantly affects young to middle-aged women, with exacerbations and remissions of disease. Seborrheic blepharitis is seen in a somewhat older age group, with an equal incidence in men and women.3 Posterior blepharitis involves the posterior lid margin and is characterized by meibomian gland dysfunction, sometimes associated with rosacea. Meibomian glands are enlarged sebaceous glands aligned in a row posterior to the eyelashes. They produce a clear lipid secretion that makes up the outer layer of the tear film. All forms of blepharitis may result in a disruption of the ocular surface, exacerbate dry eye syndrome, and result in the development of hordeola or chalazia. A chalazion is a chronic, sterile, lipogranulomatous inflammatory lesion of the meibomian gland, whereas a hordeolum is an acute infection of one of the glands in the eyelid. The most commonly associated organism is Staphylococcus aureus. Anterior staphylococcal blepharitis is thought to be caused by an abnormal cell-mediated response to S. aureus, ultimately resulting in lid margin inflammation. Anterior seborrheic blepharitis is associated with generalized seborrhea that may involve the scalp, nasolabial folds, skin behind the ears, and sternum. Posterior blepharitis is caused by meibomian gland dysfunction and alterations in meibomian gland secretions. Bacterial lipases may result in formation of free fatty acids, increasing the melting point of the meibum and preventing its expression from the glands, possibly enabling growth of S. aureus and the development of a hordeolum.4 Certain persons may be predisposed to this condition, and hormones may play a role in creating an environment that promotes lipase-producing bacteria that alter glandular secretion.5 Once the meibomian gland is obstructed from excessive meibomian oil secretions or solidification of the meibum, a chalazion or hordeolum may develop (commonly referred to as a stye). Symptoms of blepharitis are often caused by ocular tear film instability and dry eye. Patients complain of burning, foreign body sensation, tearing, photophobia, itching, redness, discharge, and swollen erythematous eyelids, often worse in the morning.6 Remissions and exacerbations are characteristic. A hordeolum or chalazion may occur at any age as a gradually enlarging localized nodule (Fig. 72-1). A hordeolum is usually painful, whereas a chalazion does not normally cause pain. Both may cause cosmetic disfigurement and mechanical ptosis. If large, the lesion may mechanically press on the corneal surface to induce astigmatism and blurred vision.7 The patient’s face, ocular adnexa, and eye should be carefully inspected. Patients with staphylococcal blepharitis may have lid margin erythema with fine ulceration at the base of the lashes and collarettes of fibrin along the lash. Lashes may be absent, broken, or misdirected. Patients with seborrheic blepharitis may have greasy scales along the lid margin and lashes with excess oily meibomian secretion and foamy tears. These patients may also have diffuse seborrhea with dandruff of the scalp and scaling of the brows, behind the ears, and at the base of the nose. Patients with posterior blepharitis may have hyperemia and telangiectasis of the lid margin (Fig. 72-2) and an oily and frothy tear film. Pressure on the lid margin results in expression of thick inspissated secretions. Rosacea is commonly associated with meibomian gland dysfunction, so these patients should be inspected for erythema with telangiectasis over the cheeks and nose, a pustular skin eruption, and sebaceous gland hypertrophy typified by rhinophyma.3 All types of blepharitis may also cause conjunctival injection, corneal infiltrates, excess tearing, lid crusting, discharge, and inflammation of the lid margin (see Fig. 72-2). When a patient with a hordeolum or chalazion is examined, the lid should be palpated for swelling and masses, and the eyelid should be everted. Hordeola and chalazia are often clinically indistinguishable. However, a hordeolum is often acute, tender, warm, and erythematous, whereas a chalazion is more chronic and nontender.
Blepharitis, Hordeolum, and Chalazion
Definition and Epidemiology
Pathophysiology
Clinical Presentation
Physical Examination





Full access? Get Clinical Tree


