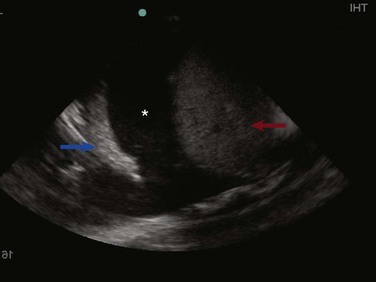
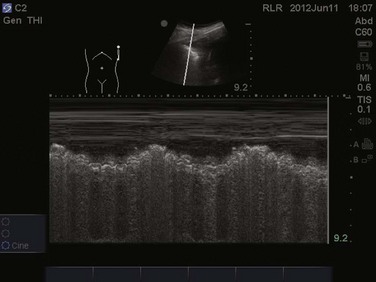
83 Lung ultrasonography is a valuable tool in the assessment of critically ill patients. The diagnostic accuracy of using ultrasound in the lung to establish the presence of pneumothorax, pleural effusion, lung consolidation, and alveolar-interstitial syndrome has been well established.1 Lung ultrasonography can be rapidly performed at the bedside and has been shown to significantly aid in the management of critical patients.2 Lung computed tomography (CT) remains the gold standard for thoracic imaging in the critical care setting, despite its major drawbacks (radiation, cost, transportation), even though portable chest radiography is the most common diagnostic imaging modality.2–4 Although portable chest radiographs are routinely performed in the ICU, multiple studies have shown limited diagnostic accuracy, with the elimination of routine chest radiographs having no adverse effect on length of stay, readmission, and mortality rates.5–7 Routine use of bedside lung ultrasound in the ICU has been shown to significantly reduce the number of both chest radiographs and CT scans obtained.8 In normal lung, ultrasound waves are reflected off gas-filled structures, limiting the visualization of lung structures beyond the pleura.1 The diagnosis of lung disease by ultrasound largely relies on the detection of ultrasound artifacts. To examine the thorax, a high-frequency linear transducer (5-12 MHz) is best used to visualize the relatively superficial pleural line. Lower frequency microconvex and convex transducers (2-5 MHz) can be used to scan the deeper lung parenchyma.9 Supine positioning is most commonly utilized in the ICU, and lateral decubitus positioning may assist in the visualization of the dorsal aspects of the lower lobes. To perform lung ultrasonography the transducer should be placed in a longitudinal axis, between two ribs. In this view the pleural interface can be seen as a hyperechoic horizontal line approximately 0.5 cm deep, relative to the anterior border of the ribs1,10 (Fig. 83.1). This image of the ribs and pleural line is the basic landmark in lung sonography and is often referred to as the bat sign.10,11 Pneumothorax, defined as a collection of air between the visceral and parietal pleural layers, has a frequency of approximately 6% in the ICU setting.12 Although screening for pneumothorax with supine anteroposterior (AP) chest radiography is still common in the critical care setting, sensitivities for the diagnosis of pneumothorax average 50%.13 The sensitivity for diagnosis of pneumothorax by lung ultrasound has been shown to be greater than 95% in multiple large prospective studies.14 Moreover, lung ultrasound for pneumothorax can be completed in an average of 2 to 3 minutes, significantly faster than obtaining a portable chest radiograph or transport to CT scan.15 The examination should begin with the transducer placed longitudinally at the midclavicular line at the level of the second to third intercostal space. Sequential movement of the transducer inferior and lateral across multiple rib interspaces will allow for a comprehensive examination of the pleura.9 This approach should then be repeated on the opposite hemithorax. Focusing on the pleural line in real time, a sliding type of motion of the visceral and parietal pleura can be observed. This dynamic motion is termed lung sliding, and can be seen in normal lung ultrasound ( Figure 83.5 M-mode ultrasound imaging of the lung point, correlating with the lateral edge of the pneumothorax. Two linear artifacts arising from the pleural line are key to the evaluation of pneumothorax by lung ultrasound, A and B lines. A lines are a reverberation artifact of the parietal pleura, represented as horizontal lines in a repetitive pattern (Fig. 83.6). B lines, or comet tails, are described as vertical lines extending the length of the screen, which erase A lines and move with lung sliding12 (Fig. 83.7). In lung ultrasound, the appreciation of only one B line indicates normal apposition of the parietal and visceral pleura and rules out pneumothorax at that location.9 Because A lines arise from the parietal pleura, their presence can be appreciated in both normal lung and pneumothorax. The absence of lung sliding with the presence of A lines has a sensitivity of 95% and specificity of 94% in the diagnosis of pneumothorax.12 Alveolar consolidation, seen in pulmonary edema, bronchopneumonia, lung contusion, and lobar atelectasis, results in the loss of lung aeration replaced by fluid, allowing for ultrasound transmission and imaging.1 As the ratio of lung tissue to air increases, lung hepatization appears on ultrasound imaging, with the lung parenchyma taking a hepatic tissue-like appearance3 (Fig. 83.8). Consolidated lung adjacent to the pleura will permit the transmission of ultrasound waves. A prospective clinical study in a medical ICU setting showed that 98% of alveolar consolidations abutted the pleura, allowing for ultrasound assessment. The deep border of alveolar consolidations will typically have an irregular appearance, sometimes referred to as the shred sign, unless the entire lobe is involved.10 Using CT as the gold standard, ultrasound has a 90% sensitivity and 98% specificity in the diagnosis of alveolar consolidation.18 Air bronchograms can be visualized within consolidated lung as bright highly reflective echogenic lines.21 Dynamic air bronchograms move centrifugally during inspiration and can typically be seen in pneumonia, as opposed to static air bronchograms of atelectasis.19 Alveolar-interstitial syndrome is a common entity in the ICU, caused acutely by a variety of conditions, including ARDS, acute pulmonary edema, and interstitial pneumonia.20 Interstitial edema precedes alveolar edema and may be difficult to discern on chest radiograph. Interstitial edema can be visualized on lung ultrasound by demonstrating three or more B lines located between two ribs, defined as lung rockets21 (Fig. 83.9 and The prevalence of pleural effusion is approximately 60% in the ICU setting.24 Pleural effusion may arise from a variety of conditions, most commonly heart failure, atelectasis, pneumonia, and volume overload. Portable supine chest radiography has poor sensitivity and specificity in the diagnosis of a pleural effusion, but lung ultrasound outperforms both chect radiography and clinical examination. Lung ultrasound can help differentiate pleural effusions from infiltrate or atelectasis, with a sensitivity of 92% and specificity of 93%.22 Pleural effusions appear as an anechoic area in dependent lung regions (Figs. 83.10 and 83.11). Transudative fluid appears echo-free, and exudative fluid may contain small echogenic debris. In intercostal imaging, pleural effusions will be bordered laterally by rib shadows, superiorly by the parietal pleural line, and inferiorly by the lung line. M-mode analysis demonstrates a decrease in the interpleural distance with inspiration, known as the sinusoid sign10 (Fig. 83.12). Lung ultrasound can also help estimate volume of pleural fluid. An anteroposterior diameter greater than 5 cm measured at the lung base or fifth intercostal space predicts a pleural effusion fluid volume of greater than 500 mL.25 The utilization of ultrasound to determine needle placement in thoracentesis has been shown in multiple studies to significantly decrease complication rates, especially that of pneumothorax.26–28 Localization of fluid above the diaphragm should be the first objective, avoiding mistaking peritoneal for pleural fluid.28 Once pleural fluid is visualized, the transducer should be moved one interspace above and below to evaluate the extent of the effusion.29 The chest should be scanned in both the longitudinal and cross-sectional plane and the positions of the heart, diaphragm, and liver/spleen determined. Next, an interpleural measurement (parietal pleura to visceral pleura) of at least 1.5 cm during inspiration should be obtained to allow for safe needle puncture. The potential site of needle puncture should be observed throughout the entire respiratory cycle to evaluate for the appearance of lung, heart, liver, or spleen in the projected needle path.28 After a safe site has been identified, the skin should be marked and disinfected. It is essential the patient remain in the same position as when the ultrasonography was performed.30 Real-time guidance is not necessary for needle puncture, but needle insertion should occur within minutes of ultrasound marking.31 Paracentesis is a commonly performed procedure in the critical care setting. Bedside ultrasonography prior to every paracentesis improves both the safety and efficacy of this procedure.32,33 An emergency department study comparing ultrasound-assisted paracentesis versus traditional blind technique showed a 95% success rate with ultrasound guidance versus only 61% with the traditional technique. Moreover, 25% of patients randomized to the ultrasound-assisted technique completely avoided the procedure due to either the absence of ascitic fluid or too little ascitic fluid for aspiration. Two more patients in this group did not receive paracentesis after performance of bedside ultrasound, which revealed a large cystic mass in the left lower quadrant of one patient and a ventral hernia in the other, both of which were mistaken for ascitic fluid and in which performance of paracentesis would have been potentially disastrous.33 A low-frequency curved array transducer is preferred. As with the traditional blind technique, the urinary bladder should be decompressed and the patient should be lying supine. Ascites will appear as anechoic fluid within the peritoneal cavity and often loops of bowel will be seen floating within this fluid (Fig. 83.13
Bedside Ultrasonography in the Critical Care Patient

Lung Ultrasonography
Technique and Equipment
Pneumothorax
 Video 83.1). In the presence of a pneumothorax, air is trapped between the visceral and parietal pleural layers and the dynamic motion of lung sliding will not be detected (
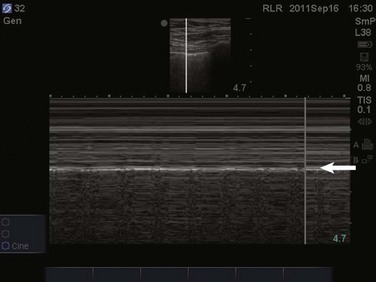
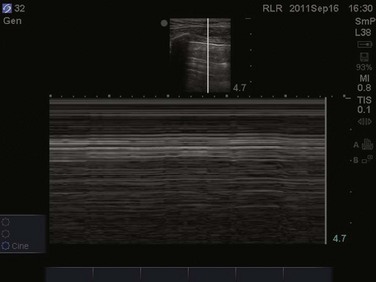
Video 83.1). In the presence of a pneumothorax, air is trapped between the visceral and parietal pleural layers and the dynamic motion of lung sliding will not be detected ( Video 83.2). The presence of lung sliding alone has a 100% negative predictive value in the diagnosis of pneumothorax.16 However, the absence of lung sliding does not rule in the diagnosis of pneumothorax. A number of conditions can result in the absence of lung sliding such as massive atelectasis, acute respiratory distress syndrome (ARDS), pleural adhesions, and severe fibrosis.9,10 M-mode and power Doppler may be useful when lung sliding is difficult to visualize on real-time B-mode imaging. M-mode analysis of normal lung tissue displays the “seashore sign,” a characteristic linear wave pattern representing the motionless chest wall, and below the pleural line a granular pattern represents normal lung motion17 (Fig. 83.2). M-mode analysis of a pneumothorax demonstrates the “stratosphere sign,” a characteristic appearance of exclusively linear lines10 (Fig. 83.3). Power Doppler will depict motion along the pleural interface, corresponding to normal lung sliding (Fig. 83.4). In the presence of a pneumothorax, no Doppler signal will be detected along the pleural surface. The visualization of the lung point may also be used in the diagnosis of pneumothorax, having a specificity of 100%. The lung point represents the area on the chest wall where normal lung sliding is again appreciated, corresponding to the lateral edge of the pneumothorax (Fig. 83.5). This confirms the absence of visualization of lung sliding was not due to technical errors in lung ultrasound, but rather the presence of pneumothorax.10
Video 83.2). The presence of lung sliding alone has a 100% negative predictive value in the diagnosis of pneumothorax.16 However, the absence of lung sliding does not rule in the diagnosis of pneumothorax. A number of conditions can result in the absence of lung sliding such as massive atelectasis, acute respiratory distress syndrome (ARDS), pleural adhesions, and severe fibrosis.9,10 M-mode and power Doppler may be useful when lung sliding is difficult to visualize on real-time B-mode imaging. M-mode analysis of normal lung tissue displays the “seashore sign,” a characteristic linear wave pattern representing the motionless chest wall, and below the pleural line a granular pattern represents normal lung motion17 (Fig. 83.2). M-mode analysis of a pneumothorax demonstrates the “stratosphere sign,” a characteristic appearance of exclusively linear lines10 (Fig. 83.3). Power Doppler will depict motion along the pleural interface, corresponding to normal lung sliding (Fig. 83.4). In the presence of a pneumothorax, no Doppler signal will be detected along the pleural surface. The visualization of the lung point may also be used in the diagnosis of pneumothorax, having a specificity of 100%. The lung point represents the area on the chest wall where normal lung sliding is again appreciated, corresponding to the lateral edge of the pneumothorax (Fig. 83.5). This confirms the absence of visualization of lung sliding was not due to technical errors in lung ultrasound, but rather the presence of pneumothorax.10

Lung Consolidation
Alveolar-Interstitial Syndrome
 Video 83.3). B lines 7 mm apart correspond to thickened interlobular septa and extravascular lung volume, but B lines 3 mm apart or less correspond to alveolar edema and a ground-glass appearance of the lung.22 In an acutely dyspneic patient, the detection of lung rockets allows the intensivist to immediately differentiate acute pulmonary edema from chronic obstructive pulmonary disease (COPD). Lung rockets are also unusual in the presence of pulmonary embolism.10 It is important to remember that B lines may be isolated or confined laterally in the last intercostal space in normal healthy lung.23
Video 83.3). B lines 7 mm apart correspond to thickened interlobular septa and extravascular lung volume, but B lines 3 mm apart or less correspond to alveolar edema and a ground-glass appearance of the lung.22 In an acutely dyspneic patient, the detection of lung rockets allows the intensivist to immediately differentiate acute pulmonary edema from chronic obstructive pulmonary disease (COPD). Lung rockets are also unusual in the presence of pulmonary embolism.10 It is important to remember that B lines may be isolated or confined laterally in the last intercostal space in normal healthy lung.23
Pleural Effusion
Thoracentesis
Abdominal Ultrasonography
Paracentesis
Related posts:

Full access? Get Clinical Tree


Bedside Ultrasonography in the Critical Care Patient