Figure 87-1 Bartholin abscess.
What To Do:
 If the swelling and pain is mild without fluctuance (bartholinitis) or if the abscess is small, the patient can be placed on antibiotics, such as metronidazole (Flagyl), 500 mg bid × 7 days, or clindamycin (Cleocin), 300 mg qid × 7 days, and instructed to take warm sitz baths. Early follow-up should be provided. If there is any risk for a sexually transmitted disease (STD) that cannot be ruled out with rapid testing, give azithromycin (Zithromax), 1 g orally in a single dose, or oral doxycycline, 100 mg twice a day for 7 days. Also give ciprofloxacin (Cipro), 500 mg orally in a single dose.
If the swelling and pain is mild without fluctuance (bartholinitis) or if the abscess is small, the patient can be placed on antibiotics, such as metronidazole (Flagyl), 500 mg bid × 7 days, or clindamycin (Cleocin), 300 mg qid × 7 days, and instructed to take warm sitz baths. Early follow-up should be provided. If there is any risk for a sexually transmitted disease (STD) that cannot be ruled out with rapid testing, give azithromycin (Zithromax), 1 g orally in a single dose, or oral doxycycline, 100 mg twice a day for 7 days. Also give ciprofloxacin (Cipro), 500 mg orally in a single dose.
 When the abscess is painful or is enlarged and presents a thin-walled segment, a 0.5- to 1-cm puncture/incision should be made with a No. 15 scalpel blade over the medial bulging mucosal surface of the labia minora and the pus evacuated. First prepare the mucosal surface with povidone-iodine (Betadine) solution and then thoroughly irrigate with normal saline or sterile water. Anesthetize the overlying tissue with 1% lidocaine (Xylocaine) with epinephrine. A No. 11 blade can be used to make the 5-mm stab incision, about 1.5 cm deep, at or behind the hymenal ring. Hold traction on the cyst with small forceps to prevent collapse of the cyst wall, and maintain visualization of the cavity.
When the abscess is painful or is enlarged and presents a thin-walled segment, a 0.5- to 1-cm puncture/incision should be made with a No. 15 scalpel blade over the medial bulging mucosal surface of the labia minora and the pus evacuated. First prepare the mucosal surface with povidone-iodine (Betadine) solution and then thoroughly irrigate with normal saline or sterile water. Anesthetize the overlying tissue with 1% lidocaine (Xylocaine) with epinephrine. A No. 11 blade can be used to make the 5-mm stab incision, about 1.5 cm deep, at or behind the hymenal ring. Hold traction on the cyst with small forceps to prevent collapse of the cyst wall, and maintain visualization of the cavity.
 After drainage, a Word catheter should be inserted through the incision. Insert it to the bottom of the cavity and inflate the tip of the catheter with approximately 1.5 to 3.0 mL of sterile water or saline to hold it in place and prevent premature closure of the opening (Figure 87-2). If balloon inflation is painful, this may indicate malplacement. Remove and reposition the Word catheter before reinflating. Also reassess the volume of inflation; a smaller amount may hold the catheter in place without maximum inflation. Balloon volumes may be larger; however, 3 mL or less likely will work well. The free end of the catheter may then be tucked up into the vagina.
After drainage, a Word catheter should be inserted through the incision. Insert it to the bottom of the cavity and inflate the tip of the catheter with approximately 1.5 to 3.0 mL of sterile water or saline to hold it in place and prevent premature closure of the opening (Figure 87-2). If balloon inflation is painful, this may indicate malplacement. Remove and reposition the Word catheter before reinflating. Also reassess the volume of inflation; a smaller amount may hold the catheter in place without maximum inflation. Balloon volumes may be larger; however, 3 mL or less likely will work well. The free end of the catheter may then be tucked up into the vagina.
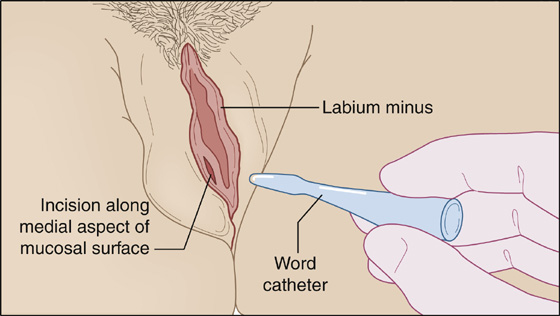
Figure 87-2 Insertion of Word catheter after incision and drainage.
 After drainage, use of prophylactic antibiotics is not recommended unless there is significant surrounding cellulitis or signs of systemic illness. One suggestion is Cefixime, 400 mg qd for 7 days, and clindamycin, 300 mg 4 times a day for 7 days. The patient should be instructed to take sitz baths and be provided with mild analgesics for the first day or two. If there is any risk for an STD, prophylaxis, as noted previously, should be administered.
After drainage, use of prophylactic antibiotics is not recommended unless there is significant surrounding cellulitis or signs of systemic illness. One suggestion is Cefixime, 400 mg qd for 7 days, and clindamycin, 300 mg 4 times a day for 7 days. The patient should be instructed to take sitz baths and be provided with mild analgesics for the first day or two. If there is any risk for an STD, prophylaxis, as noted previously, should be administered.
 Inform the patient that the catheter should stay in place for 4 to 6 weeks to allow a permanent tract to form (like a pierced ear) and thereby help prevent recurrent abscess formation.
Inform the patient that the catheter should stay in place for 4 to 6 weeks to allow a permanent tract to form (like a pierced ear) and thereby help prevent recurrent abscess formation.
 Arrange for a follow-up examination within 48 hours.
Arrange for a follow-up examination within 48 hours.
What Not To Do:
 Do not make a drainage incision on the outside of the labium.
Do not make a drainage incision on the outside of the labium.
 Do not mistake a nontender Bartholin duct cyst, which does not require immediate treatment, for an inflamed abscess.
Do not mistake a nontender Bartholin duct cyst, which does not require immediate treatment, for an inflamed abscess.
 Do not mistake a more posterior perirectal abscess for a Bartholin abscess. The perirectal abscess requires a different treatment approach.
Do not mistake a more posterior perirectal abscess for a Bartholin abscess. The perirectal abscess requires a different treatment approach.
 Do not miss an underlying malignancy, especially with an older patient with recurrent abscess formation.
Do not miss an underlying malignancy, especially with an older patient with recurrent abscess formation.
 Do not use a latex catheter in latex-allergic patients.
Do not use a latex catheter in latex-allergic patients.
Discussion
Bartholin glands are epithelial secretory glands commonly paired within the labia minora at approximately the 5-o’clock and 7-o’clock positions on the posterolateral aspect of the vestibule. Normally pea-sized and draining through a 2.5-cm duct into a fold between the hymenal ring and the labium, obstruction of the gland at the ostium can cause the glands to become cystic and subsequently form abscesses.
Simple incision and drainage without Word catheter placement may be inadequate and lead to a considerable number of recurrences of abscesses. The Word catheter is an inflatable latex balloon on the tip of a 10-Fr, 5-cm, single-barreled catheter designed to retain itself in the abscess cavity for 4 to 6 weeks to help ensure the development of a wide marsupialized opening for continued drainage. It seldom stays in place that long. The size of the incision should be kept less than 1 cm. If the incision is too large when using a Word catheter, the balloon may not be large enough, and this would increase the risk of having it fall out prematurely.
Iodoform or plain ribbon gauze can be inserted into the incised abscess as a substitute. If a wide opening persists, recurrent infections are not likely to occur, but they are common if the stoma closes.
The most common organisms involved in the development of a Bartholin abscess are anaerobic and most commonly include Bacteroides fragilis and Peptostreptococcus. Escherichia coli can also be present. About 10% to 15% of the time, Neisseria gonorrhoeae is the causative agent. Bilateral infections are more commonly characteristic of gonorrhea. Chlamydia trachomatis is involved less frequently. Often, infections are mixed.
Related posts:

Full access? Get Clinical Tree


