CHAPTER 42
Avulsed Tooth, Dental Subluxation, Dental Luxation
Presentation
After a direct blow to the mouth, the patient, usually a child 7 to 9 years old, may have a permanent tooth that has been completely knocked out of its socket (avulsion) (Figure 42-1). The tooth is intact down to its root, from which hangs the delicate periodontal ligament that used to be attached to alveolar bone. Alternatively, the tooth may have only become loosened within its normal anatomic position (subluxation) or partially displaced laterally, partially extruded from the socket, or intruded into the alveolar ridge (luxation) (Figure 42-2). These disfiguring, hemorrhagic injuries are often dramatic and a frightening experience for the patient, his parents, and other bystanders.
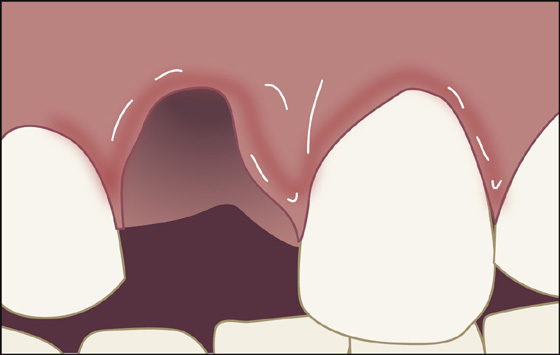
Figure 42-1 The site of an avulsed tooth. (Adapted from Honsik KA: Emergency treatment of dentoalveolar trauma. Physician Sports Med 32:23-29, 2004.)
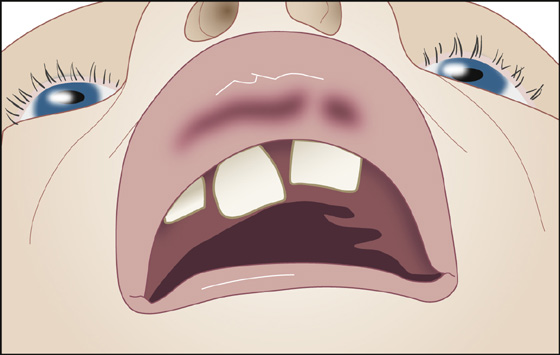
Figure 42-2 A partially extruded and laterally displaced tooth (luxation). (From Honsik KA: Emergency treatment of dentoalveolar trauma. Physician Sports Med 32:23-29, 2004.)
What To Do:
 Reassure everyone that you will be doing everything that can be done to save the patient’s tooth (or teeth) and provide comfort.
Reassure everyone that you will be doing everything that can be done to save the patient’s tooth (or teeth) and provide comfort.
 Obtain a detailed history that includes the mechanism of injury, conditions that may have led to dental contamination, the length of time that any avulsed tooth has been out of its socket, and how that tooth was stored and handled. Determine whether there are any missing teeth that cannot be accounted for and also determine if the injured teeth were primary or permanent.
Obtain a detailed history that includes the mechanism of injury, conditions that may have led to dental contamination, the length of time that any avulsed tooth has been out of its socket, and how that tooth was stored and handled. Determine whether there are any missing teeth that cannot be accounted for and also determine if the injured teeth were primary or permanent.
 Check to see whether prophylaxis against bacterial endocarditis is required because of an implanted heart valve, abnormal native valve (leakage/blockage), congenital heart defect (ventricular septal defect [VSD], atrial septic defect [ASD], patent ductus arteriosus [PDA], complex anomaly), significant mitral valve prolapse, pacemaker, or Dacron or Teflon vascular graft or patch over cardiac defect.
Check to see whether prophylaxis against bacterial endocarditis is required because of an implanted heart valve, abnormal native valve (leakage/blockage), congenital heart defect (ventricular septal defect [VSD], atrial septic defect [ASD], patent ductus arteriosus [PDA], complex anomaly), significant mitral valve prolapse, pacemaker, or Dacron or Teflon vascular graft or patch over cardiac defect.
 Examination should include evaluation of surrounding soft tissue for lacerations (see Chapter 51), with special attention to possible embedded foreign bodies (e.g., chipped teeth). Grasp the injured teeth between your gloved fingers to see if a tooth or an entire segment of teeth (e.g., alveolar ridge fractures) is mobile.
Examination should include evaluation of surrounding soft tissue for lacerations (see Chapter 51), with special attention to possible embedded foreign bodies (e.g., chipped teeth). Grasp the injured teeth between your gloved fingers to see if a tooth or an entire segment of teeth (e.g., alveolar ridge fractures) is mobile.
 Check for malocclusion and other signs of mandibular fracture as well as any other associated injuries that might be overlooked with the distracting oral trauma.
Check for malocclusion and other signs of mandibular fracture as well as any other associated injuries that might be overlooked with the distracting oral trauma.

 If a tooth is lost and cannot be accounted for, order a chest radiograph to rule out bronchial aspiration.
If a tooth is lost and cannot be accounted for, order a chest radiograph to rule out bronchial aspiration.
 The best way to preserve a tooth that has been knocked out (avulsed) is to put it back in its socket as quickly as possible. Do not delay replanting a tooth because you are waiting for radiograph results, unless you suspect an alveolar ridge fracture. Keep in mind that more accurate dental films can be done at the time of dental follow-up.
The best way to preserve a tooth that has been knocked out (avulsed) is to put it back in its socket as quickly as possible. Do not delay replanting a tooth because you are waiting for radiograph results, unless you suspect an alveolar ridge fracture. Keep in mind that more accurate dental films can be done at the time of dental follow-up.
 Primary tooth: A primary tooth that has been avulsed should not be reimplanted. The risk of injury to the developing permanent tooth is high.
Primary tooth: A primary tooth that has been avulsed should not be reimplanted. The risk of injury to the developing permanent tooth is high.
 If the permanent tooth is only partially avulsed and is just protruding farther out of its socket than normal or is angulated, simply push it back in, using firm pressure until it sits in its proper position. If the tooth is very sensitive and painful to touch, quickly provide analgesia, using an appropriate oral nerve block (see Appendix D). To ensure that the tooth is firmly reseated, have the patient bite down hard on a piece of gauze.
If the permanent tooth is only partially avulsed and is just protruding farther out of its socket than normal or is angulated, simply push it back in, using firm pressure until it sits in its proper position. If the tooth is very sensitive and painful to touch, quickly provide analgesia, using an appropriate oral nerve block (see Appendix D). To ensure that the tooth is firmly reseated, have the patient bite down hard on a piece of gauze.
 In the field, fully extruded permanent teeth may be stored under the tongue or in the buccal vestibule between the gums and the teeth. If the patient is unconscious, the tooth can be stored in cold milk or saline solution—or, if nothing else is available, water—until a better preservation solution is available. A child’s permanent tooth might be preserved, if necessary, in the parent’s mouth.
In the field, fully extruded permanent teeth may be stored under the tongue or in the buccal vestibule between the gums and the teeth. If the patient is unconscious, the tooth can be stored in cold milk or saline solution—or, if nothing else is available, water—until a better preservation solution is available. A child’s permanent tooth might be preserved, if necessary, in the parent’s mouth.
 Place the tooth in protective solution as soon as possible after patient arrival, even before obtaining additional history. Use commercially available protective solutions, such as Hank balanced salt solution or Save-A-Tooth kit. Note: Contact-lens solution is not an appropriate storage medium.
Place the tooth in protective solution as soon as possible after patient arrival, even before obtaining additional history. Use commercially available protective solutions, such as Hank balanced salt solution or Save-A-Tooth kit. Note: Contact-lens solution is not an appropriate storage medium.
 If the tooth is contaminated, hold it by the crown only and irrigate it with normal saline. Do not rub or scrub the root surface.
If the tooth is contaminated, hold it by the crown only and irrigate it with normal saline. Do not rub or scrub the root surface.
 Replacing a tooth into its socket can be facilitated by first anesthetizing the tooth socket with a dental block (see Appendix D). After the socket is numb, irrigate the socket and gently suction out any remaining debris or blood. Once the socket is prepared in this manner, replace the tooth back into the socket.
Replacing a tooth into its socket can be facilitated by first anesthetizing the tooth socket with a dental block (see Appendix D). After the socket is numb, irrigate the socket and gently suction out any remaining debris or blood. Once the socket is prepared in this manner, replace the tooth back into the socket.
 If the permanent tooth has been out of its socket for less than 15 minutes, take it by the crown, drop it in a tooth-preservation solution (see earlier), and gently flush the socket with the same solution or normal saline. Then reimplant the tooth firmly, first checking its proper orientation. Instruct the patient to bite down hard on a piece of gauze to help stabilize the tooth. Most of the time the tooth will remain stable in the socket. If necessary, secure the tooth to adjacent stable teeth with wire, arch bars, or a temporary periodontal pack (Coe-Pak).
If the permanent tooth has been out of its socket for less than 15 minutes, take it by the crown, drop it in a tooth-preservation solution (see earlier), and gently flush the socket with the same solution or normal saline. Then reimplant the tooth firmly, first checking its proper orientation. Instruct the patient to bite down hard on a piece of gauze to help stabilize the tooth. Most of the time the tooth will remain stable in the socket. If necessary, secure the tooth to adjacent stable teeth with wire, arch bars, or a temporary periodontal pack (Coe-Pak).
 Coe-Pak is a periodontal dressing that comes in the form of a base and a catalyst. Mix together the two parts and mold the resulting paste, which will eventually set semihard, over the gingival line and between the dried teeth on both the buccal and lingual sides but not over the occlusive surface of the teeth.
Coe-Pak is a periodontal dressing that comes in the form of a base and a catalyst. Mix together the two parts and mold the resulting paste, which will eventually set semihard, over the gingival line and between the dried teeth on both the buccal and lingual sides but not over the occlusive surface of the teeth.
 If a temporary periodontal splint (Coe-Pak) or wire is not available to stabilize loose teeth, spread soft wax over palatal and labial tooth surfaces and neighboring teeth as a temporary splint. If this item is not available, there is a case report showing the use of a pliable metal nasal bridge from a respirator mask to stabilize the replanted tooth. This splint is molded to the outer surface of the teeth and then glued to the reimplanted tooth and the stabilizing adjacent teeth using 2-octyl cyanoacrylate (2-OCA; Dermabond and others) (Figure 42-3).
If a temporary periodontal splint (Coe-Pak) or wire is not available to stabilize loose teeth, spread soft wax over palatal and labial tooth surfaces and neighboring teeth as a temporary splint. If this item is not available, there is a case report showing the use of a pliable metal nasal bridge from a respirator mask to stabilize the replanted tooth. This splint is molded to the outer surface of the teeth and then glued to the reimplanted tooth and the stabilizing adjacent teeth using 2-octyl cyanoacrylate (2-OCA; Dermabond and others) (Figure 42-3).
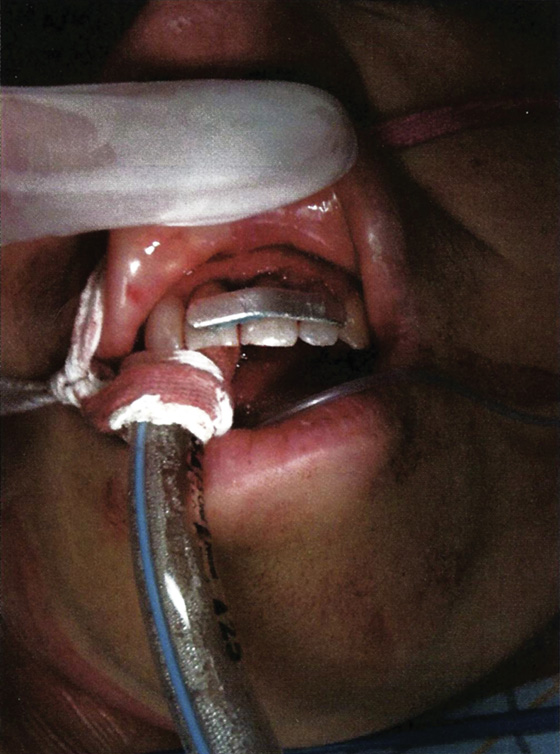
Figure 42-3 Pliable metal nasal bridge of respirator mask bonded to teeth using 2-OCA for reimplantation and stabilization of avulsed left upper central incisor (tooth 9). (Adapted from Rosenberg H, Rosenberg H, Hickey M: Emergency management of a traumatic tooth avulsion. Ann Emerg Med 57:375-377, 2011.)
 Put the patient on a soft diet, prescribe penicillin V potassium, 500 mg (12.5 mg/kg for pediatric patients) qid for 2 weeks, and schedule a dental appointment as soon as possible. Instruct the patient to brush all but the splinted teeth. Some endorse chlorhexidine mouth rinse in addition to brushing.
Put the patient on a soft diet, prescribe penicillin V potassium, 500 mg (12.5 mg/kg for pediatric patients) qid for 2 weeks, and schedule a dental appointment as soon as possible. Instruct the patient to brush all but the splinted teeth. Some endorse chlorhexidine mouth rinse in addition to brushing.
 If the permanent tooth has been out of its socket for 15 minutes to 2 hours, first soak it in the previously mentioned protective solution for 30 minutes to replenish nutrients before reimplanting. Local anesthesia will probably be needed before the tooth can be reimplanted as described earlier (see Appendix D).
If the permanent tooth has been out of its socket for 15 minutes to 2 hours, first soak it in the previously mentioned protective solution for 30 minutes to replenish nutrients before reimplanting. Local anesthesia will probably be needed before the tooth can be reimplanted as described earlier (see Appendix D).
 If the permanent tooth has been out of its socket for longer than 2 hours, the periodontal ligament is dead and should be removed, along with the pulp. Soak the tooth for 30 minutes in 5% sodium hypochlorite (Clorox) and 5 minutes each in saturated citric acid, 1% stannous fluoride, and 5% doxycycline before reimplanting. The dead tooth should ankylose into the alveolar bone of the socket as with a dental implant.
If the permanent tooth has been out of its socket for longer than 2 hours, the periodontal ligament is dead and should be removed, along with the pulp. Soak the tooth for 30 minutes in 5% sodium hypochlorite (Clorox) and 5 minutes each in saturated citric acid, 1% stannous fluoride, and 5% doxycycline before reimplanting. The dead tooth should ankylose into the alveolar bone of the socket as with a dental implant.
 Even when the tooth has been out less than 2 hours, if the patient is between 6 and 10 years of age, soak the tooth for 5 minutes in 5% doxycycline to kill bacteria that could enter the immature apex and form an abscess.
Even when the tooth has been out less than 2 hours, if the patient is between 6 and 10 years of age, soak the tooth for 5 minutes in 5% doxycycline to kill bacteria that could enter the immature apex and form an abscess.

 When consulting a dentist or an oral surgeon, the use of a dental map will help in communicating the exact tooth/teeth involved (Figure 42-4).
When consulting a dentist or an oral surgeon, the use of a dental map will help in communicating the exact tooth/teeth involved (Figure 42-4).
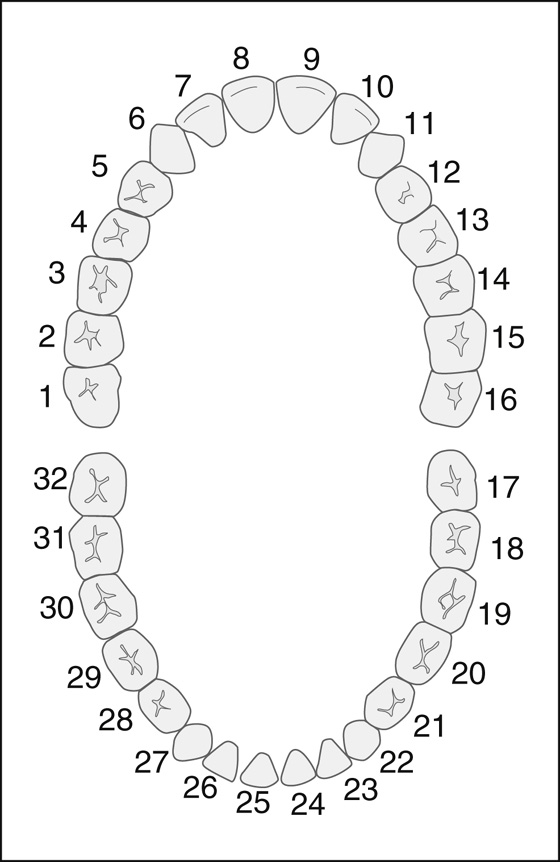
Figure 42-4 Dental map.
 Provide antibiotic prophylaxis to all patients with even minor dental trauma (e.g., subluxation) if they are at risk for bacterial endocarditis.
Provide antibiotic prophylaxis to all patients with even minor dental trauma (e.g., subluxation) if they are at risk for bacterial endocarditis.
 Consider the possibility of domestic or child abuse as the source of the trauma; if suspected, notify the appropriate authorities.
Consider the possibility of domestic or child abuse as the source of the trauma; if suspected, notify the appropriate authorities.
 Add tetanus prophylaxis to the treatment protocol if required (see Appendix H).
Add tetanus prophylaxis to the treatment protocol if required (see Appendix H).
 Inform the patient or his parents that any trauma to the teeth can lead to the death of a tooth or infection or root absorption and the eventual loss of the tooth. Also let them know that they will require dental referral for possible repositioning, more durable splinting, possible root canal therapy, and long-term follow-up. Root canal therapy will definitely be required on all permanent teeth that have been completely avulsed.
Inform the patient or his parents that any trauma to the teeth can lead to the death of a tooth or infection or root absorption and the eventual loss of the tooth. Also let them know that they will require dental referral for possible repositioning, more durable splinting, possible root canal therapy, and long-term follow-up. Root canal therapy will definitely be required on all permanent teeth that have been completely avulsed.
 Prescribe appropriate pain medication, such as oxycodone and acetaminophen (Percocet) 5 mg/325 mg, 1 to 2 tablets q4-6h prn for pain; for children 6 to 12 years old, ¼ to ½ tablet of 2.5 mg/325 mg q6h prn for pain, or for children 12 to 18 years old, ½ to 1 tablet of 2.5 mg/325 mg q6h prn for pain. Have the patient try acetaminophen or a nonsteroidal anti-inflammatory drug (NSAID) alone first to see if a narcotic is necessary. May use oxycodone oral solution 5 mg/5 mL concentration. Give 0.05 to 0.15 mg/kg PO q4-6h prn.
Prescribe appropriate pain medication, such as oxycodone and acetaminophen (Percocet) 5 mg/325 mg, 1 to 2 tablets q4-6h prn for pain; for children 6 to 12 years old, ¼ to ½ tablet of 2.5 mg/325 mg q6h prn for pain, or for children 12 to 18 years old, ½ to 1 tablet of 2.5 mg/325 mg q6h prn for pain. Have the patient try acetaminophen or a nonsteroidal anti-inflammatory drug (NSAID) alone first to see if a narcotic is necessary. May use oxycodone oral solution 5 mg/5 mL concentration. Give 0.05 to 0.15 mg/kg PO q4-6h prn.
What Not To Do:
 Do not allow an avulsed tooth to dry out. The total length of dry storage time has the greatest negative impact on the success or failure of dental reimplantation.
Do not allow an avulsed tooth to dry out. The total length of dry storage time has the greatest negative impact on the success or failure of dental reimplantation.
 Do not touch a viable root with fingers, forceps, gauze, or anything else, and do not try to scrub or clean it. The periodontal ligament will be injured and unable to revascularize the reimplanted tooth. Only hold an avulsed tooth by its crown.
Do not touch a viable root with fingers, forceps, gauze, or anything else, and do not try to scrub or clean it. The periodontal ligament will be injured and unable to revascularize the reimplanted tooth. Only hold an avulsed tooth by its crown.
 Do not overlook fractures of teeth and alveolar ridges.
Do not overlook fractures of teeth and alveolar ridges.
 Do not substitute the calcium hydroxide composition (Dycal) used for covering fractured teeth for the temporary periodontal pack (Coe-Pak) used to stabilize luxated teeth. They are different products.
Do not substitute the calcium hydroxide composition (Dycal) used for covering fractured teeth for the temporary periodontal pack (Coe-Pak) used to stabilize luxated teeth. They are different products.
 Do not reimplant an avulsed tooth if there is a complicated crown fracture, a fractured root, or an alveolar ridge fracture.
Do not reimplant an avulsed tooth if there is a complicated crown fracture, a fractured root, or an alveolar ridge fracture.
 Do not replace primary deciduous or baby teeth, although this has been done under very special circumstances. Reimplanted primary teeth heal by ankylosis; they literally fuse to the bone, which can lead to cosmetic deformity because the area of ankylosis will not grow at the same rate as the rest of the dentofacial complex. Ankylosis can also interfere with eruption of the permanent tooth.
Do not replace primary deciduous or baby teeth, although this has been done under very special circumstances. Reimplanted primary teeth heal by ankylosis; they literally fuse to the bone, which can lead to cosmetic deformity because the area of ankylosis will not grow at the same rate as the rest of the dentofacial complex. Ankylosis can also interfere with eruption of the permanent tooth.
 Do not confuse an avulsed adult tooth with a child’s deciduous tooth, which would fall out soon anyway. Normal developmental shedding of primary decidual teeth is preceded by absorption of the root. If such a tooth is brought in by mistake, there is no root to reimplant and little or no empty socket; instead, a new permanent tooth may be visible or palpable underneath.
Do not confuse an avulsed adult tooth with a child’s deciduous tooth, which would fall out soon anyway. Normal developmental shedding of primary decidual teeth is preceded by absorption of the root. If such a tooth is brought in by mistake, there is no root to reimplant and little or no empty socket; instead, a new permanent tooth may be visible or palpable underneath.
 Do not release a patient with an unsplinted tooth that is so loose that it is in danger of falling out and being aspirated.
Do not release a patient with an unsplinted tooth that is so loose that it is in danger of falling out and being aspirated.
Discussion
Accidents at home, at school, or in a motor vehicle, as well as altercations and contact sports, lead to injuries of the teeth. The maxillary central incisors are the teeth most commonly affected. When teeth are avulsed, the prognosis is best when teeth are reimplanted within 5 minutes of avulsion; yet, such optimal treatment is not always possible.
Before commercially available reconstitution solutions (e.g., Hank balanced salt solution, 320 mOsm, pH 7.2), the best treatment that could be offered the avulsed tooth was rapid reimplantation. Without a preservation solution, the chances of successful reimplantation decline approximately one percentage point every minute the tooth is absent from the oral cavity.
In mature teeth (those more than 10 years old), the pulp will not survive avulsion, even if the periodontal ligament does. At the 1-week follow-up visit with the dentist, the necrotic pulp will be removed (root canal) to prevent a chronic inflammatory reaction from interfering with the healing of the periodontal ligament.
The primary goal of rapid reimplantation is to preserve the periodontal ligament, not the tooth. With survival of the periodontal ligament, the tooth is more likely to function for a longer period of time, with less resorption of the root and reduced ankylosis.
Almost half of teeth with luxation injuries become necrotic after 3 years. The correct and timely management of these cases can increase the success of treatment.
Successful reimplantation of avulsed anterior permanent teeth can delay or negate the need for prosthetic or complex and expensive restorative procedures. Several studies have shown that teeth can function for 20 years or more after reimplantation. A number of cases have been reported in which reimplanted teeth have been functional for 20 to 40 years with a normal periodontium.

Full access? Get Clinical Tree


