Avoid Errors in Invasive Blood Pressure Measurement
Michael S. N. Hogan MB, BCh
Juraj Sprung MD, PhD
Monitoring of a patient’s blood pressure (BP) is crucial to the safe conduct of any surgical procedure. This chapter focuses on invasive arterial-line BP monitoring and some of the common errors associated with inaccurate readings.
For an arterial monitoring system to provide an accurate reading of the measured waveform, it must have an appropriate natural frequency and damping (Fig. 28.1A). Briefly, each measuring system has a natural frequency about which it oscillates. This frequency is proportional to the stiffness of the tubing and the transducer diaphragm and to the cross-sectional area of the catheter. It is inversely proportional to the catheter length and fluid density. If the frequency of the pressure wave being measured approaches the natural frequency of the system, the system distorts the measurements by excessive amplification (ringing or resonance) of the incoming waveform. This may overestimate the systolic BP by as much as 25% and underestimate the diastolic BP by 10% (the mean pressure is not affected). Damping counteracts this phenomenon.
Several problems can occur in this interaction between the natural frequency and damping parameters. Overdamping decreases the frequency response too much, underestimating the systolic BP and overestimating the diastolic BP (Fig. 28.1B). Blood clots, air bubbles in the tubing, and kinked catheters are common causes of an overdamped system. Underdamping, or hyperresonance, occurs when long connecting lines (>1.4 m) or smalldiameter tubing (<1.5 mm internal diameter) are used or when the catheter is too large for the vessel (e.g., 18-gauge catheter in a small radial artery). This overestimates the systolic BP and underestimates the diastolic BP. Underdamping may also cause the appearance of additional, small, nonphysiologic pressure waves on the tracing (Fig. 28.1C). Slow degradation in the dynamic response also may occur over time (decrease in the natural frequency with increase in the damping coefficients), causing underdamping. Fortunately, this problem can be easily rectified with periodic manual flushing of the system.
Problems within the system that lead to inaccurate measurements are usually due to problems with the mechanical connection components (i.e., the catheter, fluid-filled tubing, or the stopcock). To prevent these mechanical problems, several steps should be followed.
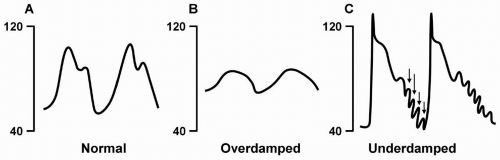 FIGURE 28.1. Arterial blood pressure (BP) waveform tracings. A: Normal. B: Overdamped tracing, causing underestimated systolic BP and overestimated diastolic BP. C: Underdamped tracing, causing overestimated systolic BP and underestimated diastolic BP. Extra nonphysiologic waveforms on the underdamped tracing reflect hyperresonance of the measuring system (arrows). |
Choose the proper size arterial cannula (20 gauge for radial or brachial, 18 gauge for femoral).
Optimize the frequency response of the measuring system by using tubing that is short (maximum length, 120 cm), wide (1.5 to 3.0 mm internal diameter), and rigid.
Use only one stopcock per line. Keep the tubing, stopcocks, and domes free of bubbles and clots. Avoid kinks in the tubing.Related posts:
 Never Neglect the Basics of Airway Management
Consider the Use of Lidocaine in the Cuff of the Endotracheal Tube, But Be Aware of the Risks and Alternatives
Do Not Underestimate the Difficulty of Reintubating a Patient Who Has Undergone Carotid Endarterectomy or Cervical Spine Surgery
Don’t Overflush Lines
Never Neglect the Basics of Airway Management
Consider the Use of Lidocaine in the Cuff of the Endotracheal Tube, But Be Aware of the Risks and Alternatives
Do Not Underestimate the Difficulty of Reintubating a Patient Who Has Undergone Carotid Endarterectomy or Cervical Spine Surgery
Don’t Overflush Lines
 Consider the Use of Tris-Hydroxymethyl Aminomethane (THAM) to Treat Refractory or Life-Threatening Metabolic Acidosis
Be Aware of the Drugs that Require Slow Intravenous Administration
Consider the Use of Tris-Hydroxymethyl Aminomethane (THAM) to Treat Refractory or Life-Threatening Metabolic Acidosis
Be Aware of the Drugs that Require Slow Intravenous Administration

Full access? Get Clinical Tree


