Aspiration of the Knee and Synovial Fluid Analysis
Bonnie J. Bidinger
Maria E. Abruzzo
Eric W. Jacobson
Arthrocentesis is a safe and relatively simple procedure that involves the introduction of a needle into the joint space to remove synovial fluid. It constitutes an essential part of the evaluation of any arthritis of unknown cause, frequently with the intent to rule out a septic process [1,2 and 3].
Ropes and Bauer [4] first categorized synovial fluid as inflammatory or noninflammatory in 1953, terms that are still used today. Hollander et al. [5] and Gatter and McCarty [6] coined the term synovianalysis to describe the process of joint fluid analysis in 1961 and were instrumental in establishing the critical role of synovial fluid analysis to diagnose certain forms of arthritis. Septic arthritis and crystalline arthritis can be diagnosed by synovial fluid analysis alone. They may present similarly but require markedly different treatments, thus necessitating early arthrocentesis and prompt synovial fluid analysis.
Indications
Arthrocentesis is performed for diagnostic and therapeutic purposes. The main indication for arthrocentesis is to assist in the evaluation of arthritis of unknown cause. In the intensive care unit, it is most commonly performed in the setting of acute monoarthritis or oligoarthritis (presenting with one to three inflamed joints) to rule out septic arthritis. Many types of inflammatory arthritis mimic septic arthritis. Synovial fluid analysis is useful in differentiating the various causes of inflammatory arthritis [4,7] (Table 19-1). Therefore, patients presenting with monoarthritis or oligoarthritis of recent onset require prompt arthrocentesis with subsequent synovial fluid analysis, preferably before initiation of treatment.
Arthrocentesis is also used for therapeutic purposes. In a septic joint, serial joint aspirations are required to remove accumulated inflammatory or purulent fluid. This allows serial monitoring of the total white blood cell count, Gram’s stain, and culture to assess response to treatment and accomplishes complete drainage of a closed space. Inflammatory fluid contains many destructive enzymes that contribute to cartilage and bony degradation; removal of the fluid may slow this destructive process [8,9]. Additionally, arthrocentesis allows for injection of long-acting corticosteroid preparations into the joint space, which may be a useful treatment for various inflammatory and noninflammatory forms of arthritis [10,11].
Before performing arthrocentesis, it must be ascertained that the true joint is inflamed and an effusion is present. This requires a meticulous physical examination to differentiate arthritis from periarticular inflammation. Bursitis, tendinitis, and cellulitis all may mimic arthritis. In the knee, the examination begins with assessment of swelling. A true effusion may cause bulging of the parapatellar gutters and the suprapatellar pouch [12]. The swelling should be confined to the joint space. To check for small effusions, the bulge test is performed [13]. Fluid is stroked from the medial joint line into the suprapatellar pouch and then from the suprapatellar pouch down along the lateral joint line. If a bulge of fluid is noted at the medial joint line, a small effusion is present (Fig. 19-1). If a large effusion is suspected, a patellar tap is performed [14]. The left hand is used to apply pressure to the suprapatellar pouch while the right hand taps the patella against the femur with sharp downward pressure. If the patella is ballottable, an effusion is probably present. Comparison with the opposite joint is helpful. Many texts describe joint examination and assessment for fluid in the knee and other joints [12,13,14 and 15].
Contraindications
Absolute contraindications to arthrocentesis, in general, include local infection of the overlying skin or other periarticular structures and severe coagulopathy [1,2 and 3,11]. If coagulopathy is present and septic arthritis is suspected, every effort should be made to correct the coagulopathy (with fresh-frozen plasma or alternate factors) before joint aspiration. Therapeutic anticoagulation is not an absolute contraindication, but every effort should be made to avoid excessive trauma during aspiration in this circumstance. Known bacteremia is a contraindication because inserting a needle into the joint space disrupts capillary integrity, allowing joint space seeding [16]. However, if septic arthritis is strongly suspected, joint aspiration is indicated. The presence of articular instability (e.g., that seen with badly damaged joints) is a relative contraindication, although the presence of a large presumed inflammatory fluid may still warrant joint aspiration.
TABLE 19-1. Common Causes of Noninflammatory and Inflammatory Arthritides | ||||
|---|---|---|---|---|
|
Complications
The major complications of arthrocentesis are iatrogenically induced infection and bleeding, both of which are extremely rare [1]. The risk of infection after arthrocentesis has been estimated to be less than 1 in 10,000 [17]. Hollander [18] reported an incidence of less than 0.005% in 400,000 injections. Strict adherence to aseptic technique reduces the risk of postarthrocentesis infection. Significant hemorrhage is also extremely rare. Correction of prominent coagulopathy before arthrocentesis reduces this risk.
Another potential complication of arthrocentesis is direct injury to the articular cartilage by the needle. This is not quantifiable, but any injury to cartilage could be associated with degenerative change over time. To avoid cartilaginous damage, the needle should be pushed in only as far as necessary to obtain fluid, and excessive movement of the needle during the procedure should be avoided.
Technique
Joint aspiration is easily learned. A sound knowledge of the joint anatomy, including the bony and soft tissue landmarks used for joint entry, is needed. Strict aseptic technique must be followed to minimize risk of infection, and relaxation of the muscles surrounding the joint should be encouraged because muscular contraction can impede the needle’s entry into the joint.
Most physicians in the intensive care unit can aspirate the knee because it is one of the most accessible joints. Other joints should probably be aspirated by an appropriate specialist, such as a rheumatologist or an orthopaedic surgeon. Certain joints are quite difficult to enter blindly and are more appropriately entered using radiologic guidance, such as with fluoroscopy or computed tomography; these include the hip, sacroiliac, and temporomandibular joints. Many texts describe in detail the aspiration technique of other joints [3,18,20,21]. The technique for knee aspiration is as follows:
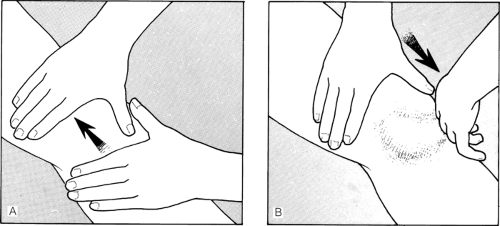 FIGURE 19-1. The bulge test. A: Milk fluid from the suprapatellar pouch into the joint. B: Slide hand down the lateral aspect of the joint line and watch for a bulge medial to the joint. |
Describe the procedure to the patient, including the possible complications, and obtain written informed consent.
Collect all items needed for the procedure (Table 19-2).
With the patient supine and the knee fully extended, examine the knee to confirm the presence of an effusion, as described previously.
Identify landmarks for needle entry. The knee may be aspirated from a medial or lateral approach. The medial approach is more commonly used and is preferred when small effusions are present. Identify the superior and inferior borders of the patella. Entry should be halfway between the borders just inferior to the undersurface of the patella (Fig. 19-2). The entry site may be marked with pressure from the end of a ballpoint pen with the writing tip retracted. An indentation mark should be visible.
Cleanse the area with 2% chlorhexidine in 70% isopropyl alcohol and allow the area to dry. Practice universal
precautions: wear gloves at all times while handling any body fluid, although they need not be sterile for routine knee aspiration. Do not touch the targeted area once it has been cleaned.
Apply local anesthesia. A local anesthetic (1% lidocaine) may be instilled with a 25-gauge, 1.5-inch needle into the subcutaneous skin. Once numbing has occurred, deeper instillation of the local anesthetic to the joint capsule can be performed. Some physicians may use ethyl chloride as an alternative anesthetic. However, this agent provides only superficial anesthesia of the skin. To use, spray ethyl chloride directly onto the designated area; stop when the first signs of freezing are evident in order to limit potential for skin damage.Related posts:

Full access? Get Clinical Tree








