Evaluation of the Patient with Acute Arthritis
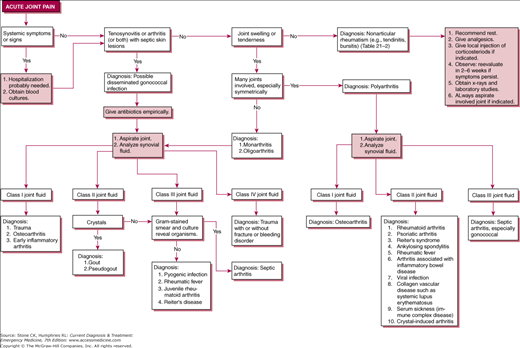
Whenever a patient with acute joint pain also presents with fever, rigors, systemic symptoms, or signs of involvement of additional organ systems, careful evaluation is necessary to rule out potentially life-threatening processes such as infection or diffuse vasculitis. Hospitalization and consultation for evaluation of rheumatic or infectious disease are usually required for patients with arthritis and systemic symptoms. Obtain blood cultures, and perform the evaluation outlined below.
In young adults, hematogenous gonococcal infection is one of the most common causes of acute arthritis. Arthritis may be the sole manifestation of disseminated gonococcal infection. Skin lesions are few and are found on the extremities, frequently around a joint, and are pustular or hemorrhagic, rarely bullous. Gram-stained smears of material contained in the pustules may reveal gram-negative diplococci within polymorphonu-clear neutrophils. Tenosynovitis classically involves tendons of the hand or foot. The primary (mucosal) site of gonococcal infection is often asymptomatic. If disseminated gonococcal infection is suspected, culture of blood and secretions from the pharynx, rectum, and urethra or cervix should be obtained.
Ascertain by careful examination whether acute joint pain is due to an intra-articular process. Is there redness, diffuse warmth, effusion, or painful limitation of active and passive motion? If the joint is not involved, consider cellulitis, tenosynovitis, bursitis, or other periarticular lesions.
Involvement of 1–3 joints in an asymmetric pattern is generally considered a characteristic of oligoarthritis, although this asymmetric involvement may occur early in some polyarticular conditions such as juvenile rheumatoid arthritis. Common causes of oligoarthritis include infection, crystal deposition (eg, gout), and trauma. The polyarthritis syndromes involve many joints, usually in a symmetric fashion.
If one of the affected joints is acrally located (eg, wrist, elbow, knee, ankle), arthrocentesis should be attempted in the emergency department, using local anesthesia and sterile technique (Chapter 6). A specialist and/or ultrasound guidance should be considered for arthrocentesis of the shoulders and hips. The joint fluid should be analyzed and the results should be used to classify the arthritis according to the scheme in Table 19–1.
See Table 21–1.
| Type of Joint Fluid | Viscosity | Clarity | Color | Leukocyte Count (per μL) | Gram Stain and Culture | Other Findings |
|---|---|---|---|---|---|---|
| Normal | High | Clear | Light yellow | <200 | Negative | … |
| Noninflammatory (class I) | High | Clear | Light yellow | <4000 | Negative | … |
| Inflammatory (class II) | Low | Cloudy | Dark yellow | >2000–<50,000 | Negative | Crystals are diagnostic of gout or pseudogout (differentiate with polarizing microscopy); usually seen with class II joint fluid |
| Septic (class III) | Low | Cloudy | Dark yellow | Usually > 50,000 | Usually positivea | Bacteria on culture or Gram-stained smear. Usually seen with class III joint fluid but may be seen with class II; rarely, class I |
| Hemorrhagic (class IV) | Variable | Cloudy | Pink-red | Usually > 2000b | Negative | Fat globules strongly suggest intraarticular fracture and are usually seen with class IV joint fluid |
Acute arthritis in the presence of normal joint fluid usually indicates trauma, or osteoarthritis. Rarely, early joint aspiration in inflammatory arthritis produces a similar result.
Inflammatory arthritis may be present in acute gout, pseudogout, Reiter syndrome, rheumatoid arthritis, and rheumatic fever. Gram stain and culture of synovial fluid should be done to rule out early infectious arthritis.
Purulent joint fluid (class III) is seen almost exclusively in bacterial and fungal infections. Gram stain of joint fluid may help to identify the causative organism before cultures become positive.
Hemorrhagic joint fluid is seen in trauma with or without fracture; the presence of fat globules suggests fracture. A tear in the anterior cruciate ligament is the most common cause of hemarthrosis in the knee when no fracture is present. Other frequent causes of hemarthrosis include peripheral meniscus tears and patellar dislocations (with medial retinaculum tears). Hemorrhagic effusion is more likely to be associated with acute pain than is the noninflammatory effusion that can occur with minor joint trauma, because blood within the joint space generally causes an inflammatory reaction. Hemorrhagic fluid is also seen in hemophilia and in synovial neoplasms.
1This chapter is a revision of the chapter by Terry C. Hermance and L. Richard Boggs, from the 6th edition.
Emergency Treatment of Specific Conditions Causing Acute Arthritis—Monarthritis or Oligoarthritis
- Effusions often develop immediately after trauma
- Fever or other systemic signs or symptoms are not present
Severe joint pain associated with trauma is usually related temporally to an obvious injury. Mild pain may occur some time after the injury. Fever and other systemic signs usually are not present. The presence of noninflammatory or hemorrhagic synovial fluid confirms the diagnosis. Because patients with septic arthritis may also give a history of recent trauma, Gram stain and culture of fluid routinely should be performed.
The presence of many small fat globules in hemorrhagic joint fluid strongly suggests intra-articular fracture; X-rays should be carefully scrutinized to locate occult fractures. Well-localized tenderness over a bone is an important sign of fracture (Chapter 28). Scaphoid fractures are particularly difficult to locate and require careful correlation with clinical findings (eg, localized tenderness in the anatomic snuffbox). X-rays that show only joint effusion or periarticular soft tissue swelling are consistent with occult fractures or other joint injuries such as spontaneously reduced dislocations, ligamentous injuries, meniscus tears, avulsion fractures, and osteochondral fractures. Joint effusions that accumulate immediately following trauma are uniformly hemorrhagic and usually do not require arthrocentesis for diagnostic purposes.
Splinting, protection from weight bearing, and follow-up care are essential. Analgesia may be needed. See Chapter 28 for more specific details and guidelines for treatment and disposition.
- Presence of negative birefringent urate crystals in joint fluid and a negative Gram stain and culture
- Uric acid level is not helpful for diagnosis in an acute attack
Patients with acute gouty arthritis have monarthritis or oligoarthritis with class II or class III joint fluid, urate crystals in the synovial fluid, and a negative synovial culture.
There is sudden onset of warmth, hyperemia, induration, and extreme pain in a joint, most commonly the metatarsophalangeal joint of the great toe. The next most commonly involved joint is the knee. Although most patients present with only one painful joint, several joints may be involved.
Elevated serum uric acid concentration is supporting evidence of gouty arthritis, although during an acute attack the serum urate level may be normal. Therefore, a uric acid level should not be ordered. Definitive diagnosis requires use of a polarizing microscope to demonstrate characteristic negative birefringence of urate crystals in the synovial fluid.
Indomethacin or other nonsteroidal anti-inflammatory drugs (NSAIDs) may be indicated if a diagnosis of gout is well established. Aspirin is contraindicated, because small doses may cause hyperuricemia.
Give 50 mg orally every 8 hours for 2 days. Then reduce the dosage to 25 mg 3–4 times daily for 3 days. Peptic ulcer disease is a contraindication to indomethacin.
Alternatives to indomethacin include ibuprofen 600 mg orally every 6 hours, naproxen 500 mg orally every 12 hours, may be used. Other NSAIDs, such as ketoralac in appropriate doses, can also be effective in acute gout.
Oral or intravenous colchicine, if administered within 24 hours of acute arthritis, can provide dramatic relief. Colchicine should not be used in patients with renal or hepatic dysfunction. Response to colchicine also strongly supports a diagnosis of gout.
Give colchicine, 0.6 mg every hour until pain has resolved, a maximum dose of 4–6 mg is reached, or side effects of nausea and diarrhea cannot be tolerated.
Gastrointestinal toxicity can be reduced by giving colchicine, 1–2 mg intravenously in 50 mL of normal saline over 20 minutes; repeat this dose every 6 hours until the patient is asymptomatic or to a total dose of 4 mg. After a full course of colchicine, no further doses should be administered for 1 week.
Corticosteroids are useful in patients who cannot take NSAIDs or colchicine. Prednisone, 40 mg daily for 1–3 days followed by a slow taper over 1–2 weeks, is recommended. Alternatively, a single dose of adrenocorticotropic hormone or corticotrophin, 40 units intramuscularly, boosts the patient’s endogenous steroid production and can provide relief from a gouty flare-up.
Hospitalization is rarely necessary. The patient should receive follow-up evaluation in a few days.
- Calcium pyrophosphate crystals in the joint
Patients with acute pseudogout have acute oligoarthritis with class II joint fluid and calcium pyrophosphate crystals in the synovial fluid. Pseudogout simulates gout in middle-aged or elderly patients. It differs from gout in that the knee is the most commonly involved joint.
Serum uric acid levels are usually normal. Chondrocalcinosis may be present, although not necessarily in the acutely involved joint. The presence of chondrocalcinosis, however, regardless of location, is not diagnostic. Definitive diagnosis depends on the presence of calcium dihydrate (pyrophosphate) crystals in synovial fluid.
Aspiration of the joint is often adequate for relief of symptoms. NSAIDs may be helpful (see Acute Gouty Arthritis, above). Unlike patients with gouty arthritis, patients with acute pseudogout do not respond as well to colchicine.
Hospitalization is rarely necessary. Refer the patient to a primary care physician.
- Joint is painful, erythematous, and tender
- Systemic symptoms: fever and chills are common
- Definitive diagnosis by aspiration of the joint. Fluid may demonstrate the infecting organism by Gram stain or culture
Septic arthritis is one of the more common causes of oligoarthritis, but often only one joint is affected. The most frequent pathogen in septic oligoarthritis is the gonococcus, which, although difficult to demonstrate in joint fluid, often produces typical pustular skin lesions or tenosynovitis. The most common pathogen in monarticular septic arthritis is Staphylococcus aureus. Another common pathogen is Streptococcus spp. In intravenous drug users and immunocompromised hosts, gram-negative and anaerobic organisms may be seen.
Patients with septic arthritis show evidence of infection in the joint (bacteria on Gram-stained smear or culture, or rapid response to antimicrobial therapy). Class III joint fluid is usually present.
Patients with septic arthritis usually present with a severe monarticular process characterized by marked pain, erythema, and tenderness. The onset of septic arthritis is usually less precipitous than that of gout. A few patients with staphylococcal or gonococcal arthritis may present with two or more involved joints. Acute migratory oligoarthritis followed in 1–2 days by acute arthritis localized to one or two joints is especially suggestive of gonococcal arthritis. If multiple joints are involved in septic arthritis, the distribution is usually asymmetric. Systemic symptoms and signs of infection (eg, fever, chills, leukocytosis) are common.
A definitive diagnosis is established by demonstrating the infecting organism in synovial tissue or joint fluid. Joint fluid shows high leukocyte counts, usually over 50,000/mL. The higher the white blood cell count in joint fluid, the greater the likelihood of bacterial or fungal arthritis. The glucose content of synovial fluid is usually reduced. If no antimicrobial therapy has been given, smears and cultures of joint fluid usually reveal organisms.
In gonococcal arthritis, however, Gram-stained smears and even cultures of joint fluid are frequently negative, although in most cases, cultures of exudate from the cervix, urethra, pharynx, or rectum demonstrate gonococci. In gonococcal arthritis, the diagnosis may also be confirmed by prompt response to antimicrobial therapy (Chapter 42).
Aspiration of the joint is essential. Obtain cultures of blood and joint fluid. If gonococcal arthritis is suspected, cervical, urethral, and possibly pharyngeal and rectal cultures should be obtained. If sepsis is considered likely, as much fluid as possible should be removed from the joint.
Begin an antibiotic deemed appropriate based on clinical findings and Gram-stained smears. Narrow the antibiotic coverage once results of Gram stain, culture, and sensitivities are reported. The treatment of gonococcal arthritis is discussed in more detail in Chapter 42.
Hospitalize all patients with suspected or documented septic arthritis and start them on intravenous antibiotics. Consult an orthopedic surgeon for possible incision and drainage of the infected joint. Patients with mild gonococcal arthritis often can be discharged early and given antibiotics to be taken orally, provided that they are reliable patients and that careful follow-up can be ensured.
- Usually polyarticular involvement. Most commonly involves hips, knees, spine, and distal and proximal interphalangeal joints
- Systemic signs and symptoms (fever and chills) should be absent
- Radiographs usually demonstrate cartilage changes with osteophytes
Related posts:






Full access? Get Clinical Tree


