Arteritis
Michael Wall
James John Corbett
Arteritis causes headache by inflammation of dural and cerebral arteries. Arteritis is thought to be due to immune complex deposition in vessel walls. Of the many causes of arteritis, this chapter concentrates on giant cell arteritis (GCA), systemic lupus erythematosus (SLE), and primary central nervous system (CNS) vasculitis.
GIANT CELL ARTERITIS
International Headache Society (IHS) code and diagnosis: 6.4.1 Headache associated with giant cell arteritis
World Health Organization (WHO) code and diagnosis: G44.81 Headache associated with other vascular disorders
Short description: Giant cell arteritis (GCA) is a polysymptomatic disease of the elderly characterized by granulomatous inflammation of aortic origin vessels. Prominent symptoms are headache and other cranial pains, jaw claudication, visual loss, hip and shoulder girdle stiffness, and constitutional symptoms.
Other terms: Temporal arteritis, Horton’s disease, cranial arteritis
Ali ibn Isâ first described GCA in the 10th century when he noted heat and inflammation in the temporalis muscles associated with loss of sight (50). Hutchinson in 1890 described a man who had symmetric, painful red streaks on his head that prevented him from wearing his hat; he ascribed the disorder to the pressure of the hat on the temples (28). In 1932, Horton and colleagues reported on two patients with a characteristic clinical presentation for GCA. They performed the first temporal artery biopsies that showed the well-known pathologic findings (26). Jennings in 1938 emphasized the blinding ocular complications and the associated musculoskeletal symptoms now known as polymyalgia rheumatica (PMR) (29).
EPIDEMIOLOGY
The incidence of GCA is 3 per 100,000 per year in Rochester, Minnesota (16), and 9 per 100,000 per year in Göteborg, Sweden (4). GCA was found in 1.7% of 889 postmortem examinations (1). The incidence of GCA rises dramatically with increasing age after age 50, from 17.4 per 100,000 (27) to 22 per 100,000 (42); it is nine times as frequent in the ninth decade as the sixth (4). The mean age at diagnosis is about 70 years. GCA rarely is reported in patients younger than 50 years, but the diagnosis in these cases is seldom confirmed (24). GCA is rare in Asians and African Americans and is most common in northern geographic areas, especially in persons of British or Scandinavian heritage (34). GCA is two to four times more common in women than in men (39).
Ninet and colleagues summarized data on a potential genetic basis for GCA and concluded that a predisposition is probable because of the higher frequency in Caucasians and reports of familial forms (familial cases appear to be uncommon) (38). Also, an association with human leukocyte antigen (HLA) DR4 antigen was suggested (38).
PATHOLOGY
The presence of granulomatous arteritis is the sine qua non for the diagnosis of GCA. Histologic features usually include (a) patchy, granulomatous inflammation involving the vessel media with lymphocytes predominating and the presence of epithelioid cells and histiocytes that, unlike giant cells that often are seen, are necessary for the diagnosis; (b) fragmentation of the internal elastic lamina; (c) occlusion of the vessel lumen with thrombus or marked subintimal edema and cellular proliferation; and (d) areas of subintimal fibromuscular hyperplasia with lymphocytic and plasma cell infiltration of the adventitia, but their presence is nondiagnostic (2).
“Skip” areas of vessel pathology are common and represent a major cause of false-negative biopsies; thus, a segment of artery of at least 1 inch should be obtained and serial sectioned at least every 1 mm throughout its length. Direct immunofluorescence microscopy using antibodies to immunoglobulin (Ig) G, IgM, IgA, complement, and fibrinogen is usually abnormal but is not more sensitive than light microscopy (48). Humoral immunity is abnormal with the presence of circulating immune complexes in the serum and deposition of immunoglobulins in arteries. Cellular immunity also appears to be abnormal with decreased OKT 8 in the blood. Activation of CD4+ T cells in the adventitia is indicative of antigen-antibody reactivity, but it is unclear whether the antigen is of internal or external origin.
At autopsy, the superficial temporal, posterior ciliary, ophthalmic, and vertebral arteries are often involved (49), which parallels the amount of elastic tissue in the media and adventitia of the arteries of the head and neck. The internal and external carotid, central retinal, and anterior ciliary arteries are less commonly involved. Involvement of arteries after they penetrate the dura is rare. The pathologic process is similar to that of Takayasu arteritis, which led to the suggestion that Takayasu arteritis may be a related or biphasic manifestation of a similar pathogenic process.
CLINICAL FEATURES
The IHS diagnostic criteria for GCA (Revised International Classification for Headache Disorders [ICHD-II]) are as follows:
A. One or more of the following:
1. Swollen and tender scalp artery (usually superficial temporal artery)
2. Elevated red blood cell sedimentation rate
3. Disappearance of headache within 48 hours of steroid therapy
B. Temporal artery biopsy demonstrating GCA.
C. Headache as a new symptom or of a new type occurs in close temporal relation to onset of GCA.
SYMPTOMS
GCA is expressed in numerous ways (Table 110-1). Headache, jaw claudication, throat pain, and other head and neck pains are usually present. Jaw claudication or neck pain markedly increases the likelihood of a positive biopsy (18). Constitutional symptoms, nontender shoulder and hip girdle aching and stiffness, diplopia, and hair loss may be present before the occurrence of visual loss. Although postmortem studies usually show involvement of the vertebral artery, stroke is uncommon. Patients uncommonly present with few or no symptoms, a condition that is called occult giant cell arteritis. In this form, the clinical presentation is purely visual (anterior ischemic optic neuropathy, ocular motor palsies, or central retinal artery occlusion), with no systemic symptoms. It is agreed that occult GCA is due to failure to recognize symptoms by either patient or physician (23).
TABLE 110-1 Cranial Symptoms of Giant Cell Arteritis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Hutchinson’s original patient had headache that worsened when he wore a hat and had scalp ischemia with gangrene. Headache is present in up to 90% of patients and often localized to one or both temporal regions or the forehead, but it may be holocranial, spare the temple, or occur in any location (44). The pain is constant in about half of patients and intermittent in the other half (44). The pain is often described as throbbing (44) or superficial and burning with a superimposed lancinating quality (4), but it may be a boring sensation (30); its intensity ranges from mild to severe (4). The headache may be a relatively minor feature in the background of generalized aches and pains of PMR. It may be so far in the background as to be recognized only by its absence after therapy is started. Head soreness and cutaneous allodynia (increased sensitivity to touch, brushing, combing, etc.), which are unusual features of other types of headache, are important complaints of patients with GCA. With severe granulomatous inflammation, frank scalp necrosis can occur (Fig. 110-1).
The visual loss in GCA may be transient (amaurosis fugax), unilateral, or bilateral (19). When visual loss is permanent, it is due to granulomatous inflammation of the posterior ciliary arteries with anterior ischemic optic neuropathy (AION). Jaw or masticatory claudication is almost pathognomonic; it does not occur with atherosclerosis.
The pain produced by chewing is an aching cramp in the jaw or the temporalis muscle and should be differentiated from temporomandibular joint disease, which is preauricular (anterior to the tragus) and often occurs immediately upon chewing. Tongue pain or infarction of the tongue also can occur.
The pain produced by chewing is an aching cramp in the jaw or the temporalis muscle and should be differentiated from temporomandibular joint disease, which is preauricular (anterior to the tragus) and often occurs immediately upon chewing. Tongue pain or infarction of the tongue also can occur.
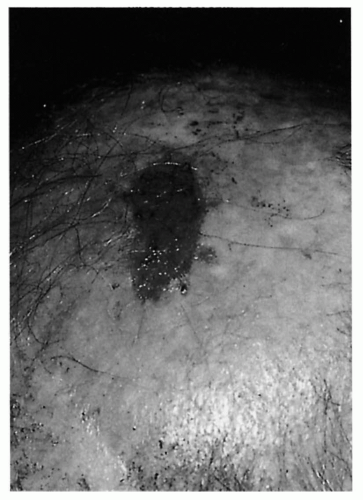 FIGURE 110-1. Scalp necrosis in a case of giant cell arteritis. (Courtesy of Mr. Roger Hitchings, Moorefields Eye Hospital.) |
PMR is a syndrome of synovial inflammation that accompanies many cases of GCA. Biopsy of the synovium shows nonspecific inflammatory changes without granulomatous arteritis. Patients have chronic stiffness of the shoulder girdles with common involvement of the sternoclavicular joint. Thickened synovium can be palpated in the sternoclavicular joint in about 40% of patients. The hip girdle is less commonly affected. The pain and stiffness are especially prominent in the morning. Proximal muscle pain may occur, but muscle biopsies are normal; the pain is thought to be referred from joints, tendons, and ligaments.
At least 20% of patients (possibly many more) with GCA have a PMR-like prodrome (15). About half of patients with PMR later develop GCA; about one fourth have serious visual or neurologic complications (30). Patients with PMR may have positive temporal artery biopsies but, according to some investigators, if they do not have any symptoms of GCA, they appear to be at low risk for visual loss. Also, low-dose corticosteroids do not protect PMR patients from developing GCA. A number of questions remain regarding the relationship of GCA and PMR, largely because of the lack of large, long-duration, prospective studies.
SIGNS
Many GCA signs are visual. Patients with AION characteristically develop pale, swollen optic discs (Fig. 110-2) with accompanying blinding visual loss. Diplopia, when present, is likely due to ischemia of the extraocular muscles (3) as a result of involvement of muscular branches of the anterior ciliary arteries. Ischemia of the third, fourth, or sixth cranial nerves probably also occurs but is rare (19). Prominent (Fig. 110-3) tender, nonpulsatile, noncompressible, or beaded temporal arteries may be present, but the artery may be normal to palpation.
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
A typical clinical course or characteristic temporal artery biopsy establishes the diagnosis of GCA. Biopsies should show interruption of the internal elastic membrane with infiltration of mononuclear cells in the arterial wall. The presence of giant cells is not required.
A 77-year-old woman presented with a 2-week history of temporal headache, fever, myalgias, fatigue, and anorexia. Erythrocyte sedimentation rate (ESR) was 125 mm per hour. At surgery, the left temporal artery was thickened. The first biopsy specimen (Fig. 110-4) showed evidence of resolution: so-called healed arteritis. A contralateral biopsy on the other side demonstrated an area of granulomatous inflammation adjacent to normal artery (Fig. 110-5).
Bengtsson and Malmvall propose that biopsy-negative patients with GCA are identified by at least one of the
following characteristic symptoms and signs: temporal ache, scalp tenderness, jaw claudication, features of AION, or abnormal temporal arteries (4). In addition, an ESR above 40 mm per hour (Westergren) and an age of 50 years or more are required, as is rapid and lasting relief of symptoms after institution of corticosteroid therapy.
following characteristic symptoms and signs: temporal ache, scalp tenderness, jaw claudication, features of AION, or abnormal temporal arteries (4). In addition, an ESR above 40 mm per hour (Westergren) and an age of 50 years or more are required, as is rapid and lasting relief of symptoms after institution of corticosteroid therapy.
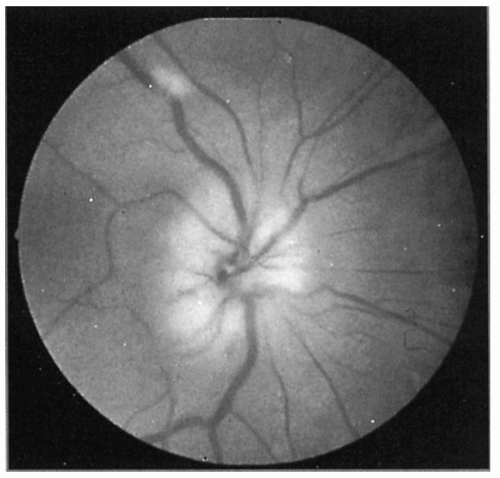 FIGURE 110-2. Pallid disk edema in giant cell arteritis. When this much pallor is present associated with disk edema in a case of anterior ischemic optic neuropathy, one should consider giant cell arteritis as a cause. (Courtesy of Sohon S. Hayreh, MD, PhD.) |
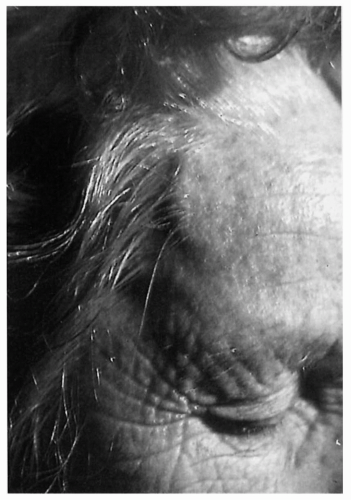 FIGURE 110-3. Prominent temporal artery in a case of giant cell arteritis.
Related posts:
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





