(1)
Chennai Breast Centre, Chennai, India
Calcifications in the breast are encountered very commonly on mammography. The vast majority of calcifications are due to benign causes. However some benign calcifications can mimic malignant calcifications and vice versa, and it becomes difficult to differentiate between the two (sometimes, malignant calcifications can appear relatively benign). It is extremely important to differentiate malignant calcifications from benign, as malignant microcalcifications are usually the only findings on a mammogram in women with ductal carcinoma in situ.
Calcifications may be formed within the ducts or lobules or outside the glandular tissue such as in the blood vessels, fat, and skin. Breast calcifications are deposits of calcium oxalate or calcium phosphate. Precipitation of these salts can occur in the fluid secreted by the epithelial cells and results in calcifications. Calcium deposits also occur in necrotic cells and tissues.
A systematic approach to detect and analyze breast calcifications will enable the radiologist to categorize and make the appropriate recommendations. Very good quality mammograms are essential to perceive the calcifications. Magnification lens with film screen mammograms or optical magnification with digital mammograms should be used to perceive calcifications. Once perceived, additional imaging should be used to optimize visualization of the calcifications for proper characterization.
Additional Views
Magnification View
Magnification view is the primary method used to further analyze the breast calcifications. It is obtained by moving the breast further away from the image receptor. As the object to image distance increases, the magnification increases by 1.5–8 times. The resulting loss of resolution is compensated by choosing a small focal spot (0.1 mm). This increases image sharpness, making it easier to analyze the morphology and the distribution of the calcifications (Fig. 8.1a, b).
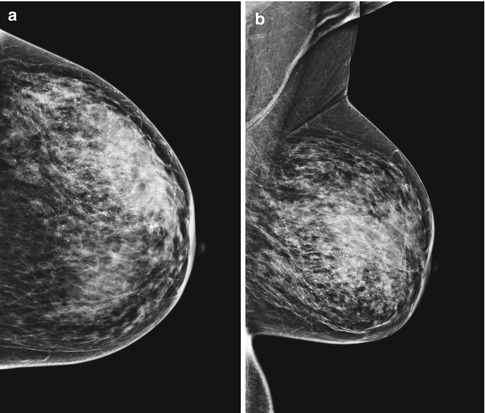
Fig. 8.1
(a, b) Image showing platform for magnification. Magnification view with air gap helps to analyze the morphology, number, and distribution of microcalcifications
The exposure time is increased with the use of a small focal spot, and this can cause motion blurring (is possible with increased exposure time). Increasing the Kv by a factor of 2 will reduce the exposure time.
Magnification views should be obtained in the craniocaudal and mediolateral projections as this will help us differentiate benign milk of calcium deposits from other calcium deposits.
A spot compression can be used along with the magnification to further improve the image quality.
True Lateral Views
True lateral views should be done to ascertain the benign nature of the calcifications. When milk of magnesia is producing the calcifications, the true lateral view allows the calcium-rich fluid to sediment at the bottom of the cystically dilated duct resulting in a meniscus sign or tea cups (Fig. 8.2a, b).
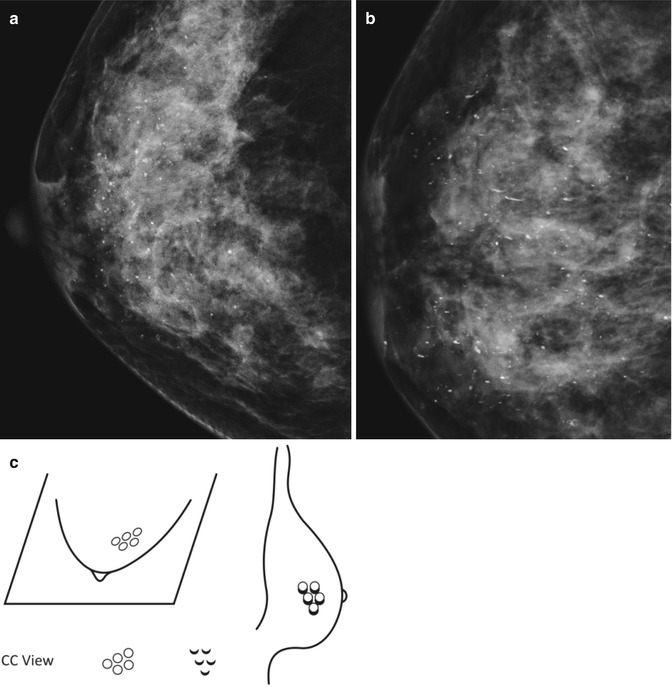
Fig. 8.2
(a) CC projection shows randomly scattered round calcifications. (b) True lateral projection shows layering down of calcifications appearing like meniscus or “tea cup.” (c) Schematics of CC and true lateral view representing “tea cup”-like calcifications
Tangential View
Tangential views are very useful to demonstrate the dermal location of the calcifications.
Systematic Approach to Analysis of Calcification
Step 1: Location
The location of the calcifications influences the morphology and distribution of the calcifications. Calcifications can develop in the skin, in the stroma, or in the ducts and acini. Calcifications that form in the acini are typically benign and appear as rosettes or like a bunch of grapes. They may also scattered and diffuse with punctate forms. Calcifications in the ducts will have a linear distribution and may have branching V and Y forms depending on the site of formation within the ducts.
Skin calcifications and masses are commonly superimposed on the breast parenchyma on screening views and mistaken for potential breast lesions. This is because only very little portion of the skin is tangent to the incident x-rays. Most of the skin is superimposed on the breast parenchyma. A tangential view helps to differentiate between a true breast lesion and the skin lesion. With skin calcifications, a CC and true lateral views are taken, and using a fenestrated compression paddle, a BB is placed at the coordinates for the calcifications, and a tangential view of the BB is obtained to show that the calcifications are in the skin (Fig. 8.3a–c).
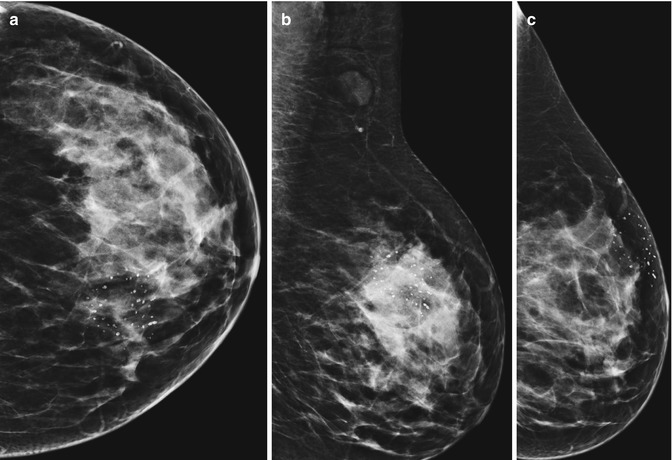
Fig. 8.3
(a, b) CC and MLO views showing group of calcifications in the upper inner quadrant with few of them showing central lucency. (c) Tangential view shows the group of calcifications lie close to the skin in the premammmary zone. This helps to differentiate a true breast calcifications from skin calcifications
Step 2: Distribution
Start Looking at Distribution
Scattered/Diffuse Calcifications
Bilateral (widely) randomly distributed calcifications throughout the breast are likely to be benign calcifications, mostly due to fibrocystic change. Some of these may be clustered also (Fig. 8.4).
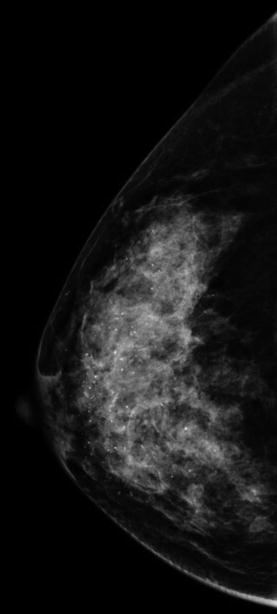
Fig. 8.4
Diffuse scattered calcification
Regional
In regional distribution, the calcifications are scattered in more than a quadrant involving a large volume of breast tissue. They are not ductal in distribution. Regional calcifications are usually representative of a benign process like fibrocystic change or sclerosing adenosis. Rarely this distribution is also noted in malignancies like DCIS (Fig. 8.5a, b).
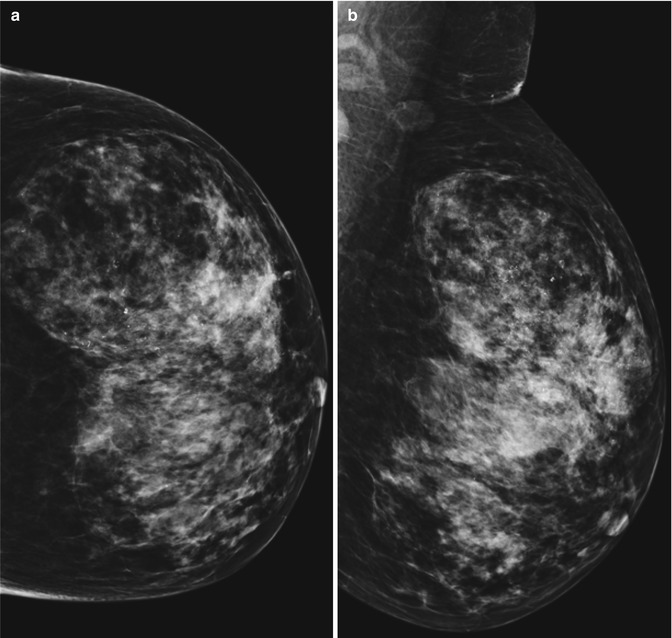
Fig. 8.5
(a, b): CC and MLO view showing regional calcifications
Segmental
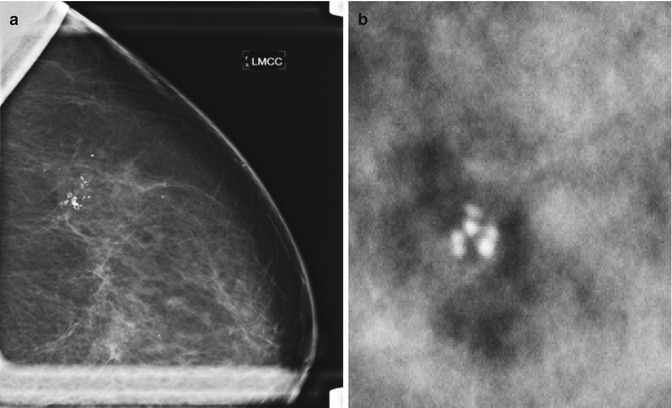
Segmental distribution usually involves one duct system with its branches in a segment or lobe. They form a triangle with the apex pointing towards the nipple. This distribution is highly suspicious for a malignancy (Fig. 8.6).
Fig. 8.6
Magnification view showing segmental distribution of the calcifications with the apex pointing towards the nipple
Grouped
A group of at least five calcifications seen in two orthogonal views within small volume of breast tissue are termed cluster of calcifications. Groups of calcifications that occur in the acini or ducts take on the shape of the anatomical structure (Fig. 8.7). When a group is identified, a spot compression and magnification views are taken. The number, size, and the forms are studied. In general, fewer than five calcifications in a cluster with round punctate forms that are 0.5 mm or less in size and are tightly packed together like a rosette or a bunch of grapes are likely to be benign (Fig. 8.7a, b). Cancer is more likely with increased number of calcifications in a group. They are more worrisome if magnification shows more in number than the standard views.