Chapter 30 Aortic Dissection
3 Describe the DeBakey and Stanford classifications of aortic dissection
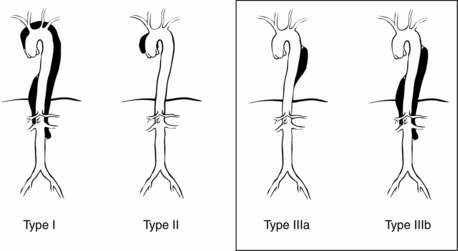
The DeBakey classification describes three types of dissection (Fig. 30-1):
 Type I: extends from aortic root to beyond the ascending aorta
Type I: extends from aortic root to beyond the ascending aorta
 Type II: involves only the ascending aorta
Type II: involves only the ascending aorta
 Type III: begins distal to the takeoff of the left subclavian artery and has two subtypes
Type III: begins distal to the takeoff of the left subclavian artery and has two subtypes


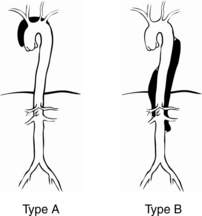
The Stanford classification has two types of dissection (Fig. 30-2):
 Type A: involves the ascending aorta
Type A: involves the ascending aorta
 Type B: involves the descending aorta, distal to the left subclavian artery
Type B: involves the descending aorta, distal to the left subclavian artery
5 What are the risk factors and associated conditions for dissection?









6 Describe the common clinical signs and symptoms of aortic dissection
 Pain: The most common presenting symptom is chest pain, occurring in up to 90% of patients with acute dissection. Classically, for type A dissections, sudden onset of severe anterior chest pain with extension to the back occurs that is described as ripping or tearing in nature. However, in the IRAD, pain was more often described as sharp rather than ripping or tearing. The pain is usually of maximal intensity from its inception and is frequently unremitting. It may migrate along the path of the dissection. The pain of aortic dissection may mimic that of myocardial ischemia. Patients with type B dissections are more likely to be seen with back pain (64%) alone.
Pain: The most common presenting symptom is chest pain, occurring in up to 90% of patients with acute dissection. Classically, for type A dissections, sudden onset of severe anterior chest pain with extension to the back occurs that is described as ripping or tearing in nature. However, in the IRAD, pain was more often described as sharp rather than ripping or tearing. The pain is usually of maximal intensity from its inception and is frequently unremitting. It may migrate along the path of the dissection. The pain of aortic dissection may mimic that of myocardial ischemia. Patients with type B dissections are more likely to be seen with back pain (64%) alone.

7 Describe the common clinical findings associated with aortic dissection
 Neurologic symptoms. The reported frequency of neurologic symptoms in pooled data of type A and B dissections approaches 17%; in type A alone, 29% of patients were seen initially with neurologic symptoms, 53% of which represented ischemic stroke. Neurologic complications may result from hypotension, malperfusion, distal thromboembolism, or nerve compression. Acute paraplegia as a result of spinal cord malperfusion has been described as a primary manifestation in 1% to 3% of patients. Up to 50% of neurologic symptoms may be transient.
Neurologic symptoms. The reported frequency of neurologic symptoms in pooled data of type A and B dissections approaches 17%; in type A alone, 29% of patients were seen initially with neurologic symptoms, 53% of which represented ischemic stroke. Neurologic complications may result from hypotension, malperfusion, distal thromboembolism, or nerve compression. Acute paraplegia as a result of spinal cord malperfusion has been described as a primary manifestation in 1% to 3% of patients. Up to 50% of neurologic symptoms may be transient.

 Acute aortic regurgitation may be present in 41% to 76% of patients with proximal dissection and may be caused by widening of the aortic annulus resulting in incomplete valve closure or actual disruption of the aortic valve leaflets from the dissection flap. Clinical manifestations of dissection-related aortic regurgitation span from mere diastolic murmurs without clinical significance to overt congestive heart failure and cardiogenic shock.
Acute aortic regurgitation may be present in 41% to 76% of patients with proximal dissection and may be caused by widening of the aortic annulus resulting in incomplete valve closure or actual disruption of the aortic valve leaflets from the dissection flap. Clinical manifestations of dissection-related aortic regurgitation span from mere diastolic murmurs without clinical significance to overt congestive heart failure and cardiogenic shock.
Full access? Get Clinical Tree


