KEY POINTS
1. The incidence of ischemia during this period has been reported to be 7% to 56%.
2. The Society of Thoracic Surgeons recommends a cephalosporin as the primary prophylactic antibiotic for adult cardiac surgery. In patients considered high risk for staphylococcus infection (either presumed or known staphylococcal colonization), it would be reasonable to combine cephalosporins with vancomycin.
3. An incidence of hypertension as high as 88% is found with sternotomy during a narcotic-based anesthetic.
4. Sternotomy is the time of the highest incidence of awareness and recall during cardiac surgery, and has been reported to be associated
5. Sinus tachycardia with heart rates greater than 100 beats/min has been associated with a 40% incidence of ischemia. Heart rate greater than 110 beats/min was associated with a 32% to 63% incidence of ischemia.
6. The most likely cause of dysrhythmia in the prebypass period is surgical manipulation of the heart.

THE PERIOD OF TIME BETWEEN induction of anesthesia and institution of cardiopulmonary bypass (CPB) is characterized by widely varying surgical stimuli. Anesthetic management during this high-risk period must strive to:
1
1. Optimize the myocardial O2 supply/demand ratio and monitor for myocardial ischemia. The incidence of ischemia during this period has been reported to be 7% to 56% [1].
2. Hemodynamics must be optimized to maintain adequate organ perfusion. This is best achieved by optimizing the preload, afterload, contractility, heart rate, and rhythm depending on the underlying cardiac dysfunction and its associated complications.
3. Manage “fast track” patients with short-acting agents.
Adverse hemodynamic changes increase the risk of developing ischemia, heart failure, hypoxemia, or dysrhythmias. These complications may alter surgical management and lead to urgent institution of CPB with failure to perform internal mammary artery (IMA) or radial artery dissection, along with an increased risk of bleeding.
A few simple rules may assist in the management of cardiac patients before CPB:
1. “Keep them where they live.”
A review of the preoperative vital signs and tests of cardiac performance (echocardiography, cardiac catheterization, and other imaging modalities) helps in guiding the management of the hemodynamics during this period.
2. “The enemy of good is better.”
If the patient’s blood pressure and heart rate are acceptable, does it matter if the cardiac index is 1.8 L/min/M2? When a patient is anesthetized, oxygen consumption decreases, so a lower cardiac index may be adequate. Trying to increase it to “normal” may lead to other problems, such as dysrhythmias or myocardial ischemia. Additional parameters such as mixed venous oxygen saturation and presence of acidosis should be considered prior to treatment.
3. “Do no harm.”
These patients are frequently very ill. If you are having problems managing the patient, ask for help.
I. Management of events before CPB
A. Stages of the pre-CPB period. The pre-CPB period can be subdivided into stages based on the level of surgical stimulation.
1. High levels of stimulation include incision, sternal split, sternal spread, sympathetic nerve dissection, pericardiotomy, and aortic cannulation. Inadequate anesthesia or sympathetic activation at these times leads to increased catecholamine levels, possibly resulting in hypertension, dysrhythmias, tachycardia, ischemia, or heart failure (Table 7.1).
Table 7.1 Typical hemodynamic responses to surgical stimulation before cardiopulmonary bypass
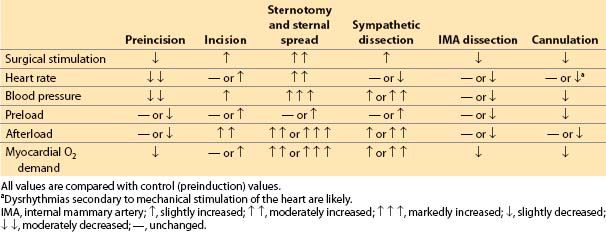
2. Low-level stimulation occurs during preincision, radial artery harvesting, internal mammary (thoracic) artery dissection, and CPB venous cannulation. Risks during these periods include hypotension, bradycardia, dysrhythmias, and ischemia (Table 7.1).
B. Preincision. This period includes surgical preparation and draping. Several parameters should be checked during this time:
1. Confirm bilateral breath sounds after final patient positioning.
2. Check pressure points. Ischemia, secondary to compression and compounded by decreases in temperature and perfusion pressure during CPB, may cause peripheral neuropathy or damage to soft tissues.
a. Brachial plexus injury can occur if the arms are hyperextended or if chest retraction is excessive (e.g., occult rib fracture using a sternal retractor) [2]. Excessive chest retraction can occur not only with the sternal spreader but also during IMA dissection even if the arms are tucked to the sides. If the arms are placed on arm boards, obtain the proper position by minimizing pectoralis major muscle tension. Do not extend arms more than 90 degrees from the body to avoid stretching the brachial plexus.
b. Ulnar nerve injury can occur from compression of the olecranon against the metal edge of the operating room table. To obtain the proper position, provide adequate padding under the olecranon. Do not allow the arm to contact the metal edge of the operating room table.
c. Radial nerve injury can occur from compression of the upper arm against the “ether screen” or the support post of the chest wall sternal retractors used in IMA dissection.
d. Finger injury can occur secondary to pressure from members of the operating team leaning against the operating table if the fingers are positioned improperly. To obtain the proper position, hands should be next to the body, with fingers in a neutral position away from the metal edge of the table. One method to prevent upper extremity injury is to have the patient position himself or herself. The patient can grasp a surgical towel in each hand to ensure that the fingers are in a comfortable and protected position.
e. Occipital alopecia can occur 3 wks after the operation secondary to ischemia of the scalp, particularly during hypothermia. To obtain the proper position, pad and reposition the head frequently during the operation.
f. Heel skin ischemia and tissue necrosis are possible. Heels should be well padded in such a way as to redistribute weight away from the heel to the lower leg.
g. The eyes should be closed, taped, and free from any pressure.
h. Commercial foam dressings may be applied prophylactically to various pressure points (sacrum and heels) to prevent pressure sores as these patients are bed ridden and may have compromised circulation.
3. Adjust fresh gas flow.
a. Use of 100% O2 maximizes inspired O2 tension. A lower inspired oxygen concentration may prevent absorption atelectasis and reduce the risk of O2 toxicity. The inspired oxygen concentration can be titrated based on pulse oximeter readings and arterial blood gases (ABGs).
b. Nitrous oxide can be used during the pre-CPB period in stable patients. It will, however,
(1) Decrease the concentration of inspired oxygen (FiO2)
(2) Increase pulmonary vascular resistance (PVR) in adults
(3) Increase catecholamine release
(4) Possibly induce ventricular dysfunction
(5) Some evidence suggests that nitrous oxide should not be used in patients with an evolving myocardial infarct or in patients with ongoing ischemia because the decrease in FiO2 and potential catecholamine release theoretically can increase the risk of ischemia and infarct size. This point remains controversial.
4. Check all monitors and lines after final patient position is achieved.
a. Intravenous (IV) infusions should flow freely, and the arterial pressure waveform should be assessed for dampening or hyper-resonance.
b. IV injection ports should be accessible.
c. All IV and arterial line connections (stopcocks) should be taped or secured to prevent their movement and minimize the risk of blood loss from an open connection.
d. Confirm electrical and patient reference “zero” of all transducers (see Chapter 4).
e. Nasopharyngeal temperature probes, if required, must be placed prior to heparinization to avoid excessive nasal bleeding.
5. Check hemodynamic status.
a. Cardiac index, ventricular filling pressures, mixed venous oxygen saturation (SvO2), and cardiac work indices should be evaluated after intubation.
b. If transesophageal echocardiography (TEE) is used, check and document the position of the probe and the presence or absence of dental and oropharyngeal injury. Make sure the TEE probe is not in a locked position, as this may lead to pressure necrosis in the gastrointestinal tract.
c. A baseline TEE examination should be performed to document the ejection fraction, wall-motion abnormalities, valve function, and shunts (see Chapter 5). The TEE probe should be placed before heparinization to avoid excessive bleeding.
6. Check blood chemistry.
a. Once a stable anesthetic level is achieved, and ventilation and FiO2 have been constant for 10 min, an ABG measurement should be obtained to confirm adequate oxygenation and ventilation, and to correlate the ABG with noninvasive measurements (pulse oximetry and end-tidal CO2 concentration). Maintain normocapnia, as hypercapnia may increase PVR. Hypocapnia may promote myocardial ischemia and cardiac dysrhythmias.
b. Mixed venous hemoglobin O2 saturation can be measured with a mixed venous blood gas at this time, if necessary, to calibrate a continuous mixed venous PA catheter.
c. Electrolytes, calcium, and glucose levels should be determined as clinically indicated. High glucose levels should be treated to minimize neurologic injury and to decrease postoperative infection rates. Intraoperative hyperglycemia is an independent risk factor for other perioperative complications, including death, after cardiac surgery [3]. Perioperative glucose management of diabetic patients must be started in the prebypass period. Glucose control may be achieved by a continuous infusion of insulin with the infusion rate depending on the patient’s blood sugar. Boluses of IV insulin may lead to large swings in blood sugar; thus, an IV infusion is preferred. It is imperative to treat the trends of blood glucose rather than absolute blood glucose levels to minimize intraoperative hypoglycemia. Thus, glycemic control should be based on the velocity of glucose change rather than an absolute value.
d. A blood sample to determine a baseline activated clotting time (ACT) before heparinization may be drawn at the same time as the sample for ABG. The blood can be taken from the arterial line after withdrawal of 5 to 10 mL of blood depending on the dead space of the arterial line tubing and avoiding residual heparin, if present, in the flush solution. The perfusionist may require a blood sample to perform a heparin dose–response curve, which in some institutions is used to determine the initial heparin dosage.
e. Before any manipulation of the arterial line (zeroing, blood sample withdrawal), it is important to announce your intentions. This avoids alarming your colleagues, who may notice the loss of the arterial waveform.
7. Antibiotics
a. Antibiotics are often administered before incision and should be timed not to coincide with the administration of other medications, should an allergic reaction occur.
b. For cardiac patients, the Surgical Care Improvement Project (SCIP) and The Society of Thoracic Surgeons (STS) Practice guidelines recommend that preoperative prophylactic antibiotics are to be administered within 1 h prior to incision with the exception of 2 h for vancomycin or fluoroquinolones and discontinued 48 h after the end of surgery for cardiac patients.
2
c. The STS recommends a cephalosporin as the primary prophylactic antibiotic for adult cardiac surgery. In patients considered high risk for staphylococcus infection (either presumed or known staphylococcal colonization), it would be reasonable to combine cephalosporins with vancomycin.
d. Exclusive vancomycin use for cardiac surgical prophylaxis should be avoided as it provides no gram-negative coverage.
e. In patients with a history of an immunoglobulin-E–mediated reaction to penicillin, vancomycin should be administered with additional gram-negative coverage [4,5].
8. Antifibrinolytics. Excessive fibrinolysis is one of the causes of blood loss following cardiac surgery. Antifibrinolytic agents are commonly used to minimize bleeding and thereby reduce the exposure to blood products.
a. Aprotinin (serine protease inhibitor). The FDA has suspended the use of aprotinin after the BART trial which demonstrated that aprotinin has a worse risk-benefit profile than the lysine analogs with a trend toward increased mortality in patients receiving aprotinin [6].
b. Epsilon-aminocaproic acid (EACA) and Tranexamic acid (lysine analogs). With the suspended use of aprotinin, EACA and tranexamic acid are the only anti-fibrinolytics available. Both are effective agents in reducing postoperative blood loss. However, EACA at equipotent doses to tranexamic acid is associated with a higher rate of temporary renal dysfunction. Tranexamic acid is associated with seizures at higher doses [7].
9. Preparation for saphenous vein excision involves lifting the legs above the level of the heart. Increased venous return increases the myocardial preload. This change is desirable in patients with low filling pressures and normal ventricular function but may be detrimental in patients with borderline ventricular reserve. Gradual elevation of the legs may be useful in attenuating the hemodynamic changes. The reverse occurs when the legs are returned to the neutral position.
10. Endoscopic saphenectomy for harvesting vein grafts for coronary artery bypass grafting is becoming common. As in a laparoscopic procedure, carbon dioxide is the insufflating gas of choice during this procedure. Mechanical ventilation may have to be adjusted depending on the rise in CO2 as detected by an end-tidal monitor and ABG analysis. When using carbon dioxide insufflation, CO2 embolism has been reported in two patients. These were associated with no untoward consequences because of prompt recognition and treatment. Frail, elderly patients with fragile tissue are at risk for this complication. Preventive measures include maintenance of a right atrial pressure to insufflation pressure gradient of greater than or equal to 5 mm Hg and addition of positive end-expiratory pressure (PEEP). Hemodynamic deterioration secondary to transmission of gas through a patent foramen ovale into the left heart and coronary circulation has also been reported [8].
11. Maintenance of body temperature is not a concern during the pre-CPB time period with the exception of off-pump coronary artery bypass grafting (OPCAB). It is preferable to allow the temperature to drift down slowly, as this allows for more homogeneous hypothermia at institution of CPB. Before CPB, increasing the room temperature, humidifying anesthetic gases, warming IV solutions, and using a warming blanket are not necessary. These measures must be available for post-CPB management. The physiologic changes associated with mild hypothermia (34 to 36°C) include the following:
a. Decrease in O2 consumption and CO2 production (8% to 10% for each degree Celsius)
b. Increase in systemic vascular resistance (SVR) and PVR
c. Increase in blood viscosity
d. Decrease in central nervous system (CNS) function (amnesia, decrease in cerebral metabolic rate or O2 consumption [CMRO2] and decrease in cerebral blood flow)
e. Decrease in anesthetic requirement (minimum alveolar concentration [MAC] decreases 5% for each degree Celsius)
f. Decrease in renal blood flow and urine output
g. Decrease in hepatic blood flow
h. Minimal increase in plasma catecholamine levels
12. Maintain other organ system function
a. Renal system [9]
(1) Inadequate urine output must be addressed immediately:
(a) Rule out technical problems first (kinked urinary catheter tubing or disconnected tubing).
(b) Optimize and maintain an adequate intravascular volume and cardiac output using central venous pressure (CVP), pulmonary artery catheter (PAC), or TEE as a measure of preload and cardiac performance.
(c) Avoid or treat hypotension.
(d) Maintain adequate oxygenation.
(e) Mannitol (0.25 g/kg IV) may be used to redistribute renal blood flow to the cortex and to maintain renal tubular flow.
(f) Dopamine (2.5 to 5 μg/kg/min) infusion may be given to increase renal blood flow by renal vascular dilation. Currently, there is no evidence that “renal” dose dopamine will prevent perioperative renal dysfunction. Its use may increase the incidence of perioperative atrial dysrhythmias.
(g) Diuretics (furosemide, 10 to 40 mg; bumetanide, 0.25 to 1 mg) can be given to maintain renal tubular flow if other measures are ineffective or if the patient had taken preoperative diuretics.
(2) Patients undergoing emergent surgery may have received a large radiocontrast dye load at angiography. Avoiding dye-induced acute tubular necrosis, utilizing the techniques mentioned earlier, is crucial.
b. CNS
(1) Adequate cerebral perfusion pressure must be maintained.
(a) The patient’s preoperative lowest and highest mean arterial pressures should be the limits accepted in the operating room to avoid cerebral ischemia. Remember “keep them where they live.”
(b) Elderly patients have a decreased cerebral reserve and are more sensitive to changes in cerebral perfusion pressure.
(2) Patients at risk for an adverse cerebral event include those with known carotid artery disease, peripheral vascular disease, or a known embolic focus. Management considerations for these patients are discussed in Chapter 22.
c. Pulmonary system
(1) Maintain normal pH, PaCO2, and adequate PaO2.
(2) Treatment of systemic hypertension with a vasodilator may induce hypoxemia secondary to inhibition of hypoxic pulmonary vasoconstriction. FiO2 may have to be increased.
(3) Use of an air–oxygen mixture may prevent absorption atelectasis.
13. Prepare for incision.
a. Ensure adequate depth of anesthesia using clinical signs. If available, a bispectral index (BIS) monitor may be helpful. A small dose of a narcotic or hypnotic or increased concentration of inhaled agent may be necessary.
b. Ensure adequate muscle relaxation to avoid movement with incision and sternotomy. If movement occurs, make sure the patient is anesthetized as you are paralyzing the patient.
C. Incision
1. An adequate depth of anesthesia is necessary but may not be sufficient to avoid tachycardia and hypertension in response to the stimulus of incision. If hemodynamic changes occur, they are usually short lived, so medications with a brief duration of action are recommended.
a. Treatment can include:
(1) Vasodilators
(a) Nitroglycerin (20- to 80-μg bolus) or infusion
(b) Sodium nitroprusside infusion
(2) β-blockers
(a) Esmolol (0.25 to 1 mg/kg)
2. Observe the surgical field for patient movement and blood color. Despite an abundance of monitors, the presence of bright red blood remains one of the best ways to assess oxygenation and perfusion.
3. If the patient responds clinically to the incision (tachycardia, hypertension, other signs of “light” anesthesia, or clinically significant BIS monitor value changes), then the level of anesthesia must be deepened before sternotomy. Do not allow sternal split until the patient is anesthetized adequately and hemodynamics are controlled.
3
D. Sternal split
1. A very high level of stimulation accompanies sternal split. The incidence of hypertension has been reported to be as high as 88% during a narcotic-based anesthetic. A cumulative dose of fentanyl, 50 to 70 μg/kg, before sternal split should decrease the incidence of hypertension to less than 50%. However, fentanyl doses greater than 150 μg/kg are necessary for further reduction in the incidence of hypertension [10]. This high dose of fentanyl, will prevent the patient from being ready for early extubation. Hypertension and tachycardia, if they occur, should be treated as described for skin incision.
Bradycardia secondary to vagal discharge can occur. It is usually self-limiting, but if it is persistent and causes hemodynamic compromise then a dose of atropine or ephedrine may be necessary.
2. A reciprocating power saw is often used to open the sternum. The lungs should be “deflated” during opening of the internal table of the sternum to avoid damage to the lung parenchyma.
3. The patient should have adequate muscle relaxation during sternotomy to avoid an air embolism. If the patient gasps as the right atrium is cut, air can be entrained owing to the negative intrapleural pressure.
4
4. This is the most common time period for awareness and recall due to the intense stimulation.
a. Awareness has been reported with fentanyl dosages as large as 150 μg/kg and with lower fentanyl doses supplemented with amnestic agents. Awareness usually, but not always, is associated with other symptoms of light anesthesia (movement, sweating, increased pupil size, hypertension, or tachycardia). A BIS monitor may be helpful, but recall has occurred in patients with an “adequate” BIS reading.
b. If an amnestic agent has not been administered previously, it should be considered before sternotomy because these agents decrease the incidence of recall but will not produce retrograde amnesia. Amnestic supplements do not always protect against the hypertension and tachycardia associated with awareness. However, amnestic supplements may cause hypotension. The most common amnestic agents, their dosages, and side effects include:
(1) Benzodiazepines (midazolam, 2.5 to 20 mg; diazepam, 5 to 15 mg; lorazepam, 1 to 4 mg) in divided doses usually are well tolerated but can decrease SVR and contractility in patients with poor ventricular function, especially when the drugs are added to a narcotic-based anesthetic.
(2) Scopolamine, 0.2 to 0.4 mg IV, may cause tachycardia if it is administered rapidly. It may prolong emergence in a “fast track” patient and it will cause pupillary dilation.
(3) Nitrous oxide may lead to catecholamine release, LV dysfunction, increased PVR, and increased risk of hypoxia. The use of nitrous oxide in noncardiac surgery (ENIGMA trial) was associated with an increased long-term risk of myocardial infarction. Nitrous oxide-induced inactivation of methionine synthetase increases plasma homocysteine levels in the postoperative period. This can lead to endothelial dysfunction and hypercoagulability. The ENIGMA-II trial is presently studying this hypothesis to ascertain the risks and benefits of using nitrous oxide [11].
(4) Inhalation agents can cause myocardial depression, bradycardia, tachycardia, dysrhythmias, or decreases in SVR, but they are effective in low concentrations and have become a standard part of the anesthetic technique to “fast track” the patient.
(5) Droperidol (0.0625 to 2.5 mg) may cause hypotension by blocking α1-receptors. This effect may last several hours.
(6) Ketamine (5 to 100 mg) can cause sympathetic stimulation unless the patient is pretreated with a narcotic or benzodiazepine.
(7) Propofol (10 to 50 mg) can cause decreased blood pressure and cardiac output.
(8) Sodium thiopental (25 to 150 mg) can cause decreased blood pressure and cardiac output.
5. Concerns with cardiac reoperation (“redo heart”)
a. The pericardium is usually not closed after heart surgery, and the aorta, RV, and bypass grafts may adhere to the underside of the sternum. At reoperation, these structures can be easily injured when the sternum is opened. A clue to this potential problem may be provided radiologically if there is no space between the heart and the inner sternal border. Although using an oscillating saw decreases this risk, it does not eliminate it. As this takes longer than the usual sternotomy, ventilation should not be held. Knowing the proximity of mediastinal structures to the sternum is necessary, and if preoperative imaging suggests that they may be in jeopardy, extra measures before reopening the sternum, such as peripheral cannulation and CPB (with or without deep hypothermic circulatory arrest), may be necessary to avoid catastrophe [12]. Venous cannulae may be passed into the right atrium through the femoral vein. The correct positioning of these cannulae may be identified on the mid-esophageal bicaval view using TEE. Axillary or subclavian cannulation may be the preferred site for peripheral arterial inflow site as compared to the femoral artery in patients with concurrent descending, thoracoabdominal, or abdominal aortic aneurysms. A discussion with the surgeon is necessary to place the arterial line for monitoring in the contralateral superior extremity in case of either subclavian or axillary cannulation. Femoral arterial cannulation may be an alternative.
b. If a graft is cut, the patient may develop profound ischemia. Nitroglycerin may be helpful, but if significant myocardial dysfunction or hypotension occurs, the ultimate treatment is prompt institution of CPB.
c. If the right atrium, RV, or great vessels are cut, a surgeon or assistant will put a “finger in the dike” while the tear is fixed or a decision is made to go emergently on CPB. CPB can be initiated using the following:
(1) “Sucker bypass” with a femoral artery cannula or aortic cannula and the cardiotomy suckers are used as the venous return line if the right atrium cannot be cannulated.
(2) Complete femoral vein–femoral artery bypass
d. The prolonged surgical dissection increases the risk of dysrhythmias.
(1) The availability of external defibrillator pads or sterile external paddles should be considered. Defibrillation may be necessary before complete exposure of the heart, rendering internal paddles ineffective.
(2) Many institutions use a defibrillation pad that adheres to the back and is placed before induction. This allows for use of an internal paddle even if the heart is not totally exposed, as current will flow in an anteroposterior fashion through the heart.
e. Volume replacement (crystalloid, colloid, blood) may be necessary to provide adequate preload if hemorrhage is brisk during the dissection.
(1) Adequate IV access for volume replacement must be available prior to the start of the surgical procedure. This may be accomplished by securing two large-bore peripheral IV lines or a large-bore multilumen central venous access catheter in a central vein.
(2) Have at least 2 units of blood available in case it is necessary to transfuse the patient.
(3) After the patient is heparinized, the surgical team should use the CPB suckers to help salvage blood.
6. Concerns with urgent or emergent cardiac operation
a. Indications include:
(1) Cardiac catheterization complications (failed angioplasty with persistent chest pain, coronary artery dissection) [13]
(2) Persistent ischemia with or without chest pain that is refractory to medical therapy or an intra-aortic balloon pump (IABP)
(3) Left main coronary artery disease or left main equivalent
(4) Acute aortic dissection
(5) Fulminant infective endocarditis
(6) Ruptured chordae tendineae
(7) Acute ischemic ventricular septal defect
(8) Multiple high-grade lesions with significant myocardium at risk
(9) Emergent LVAD placement
b. Continue blood pressure, pulse oximeter, and electro-cardiographic (ECG) monitoring during transport and preparation.
c. Aggressively treat ischemia and dysrhythmias that may be present.
d. Continue heparin infusion until sternotomy. This will increase operative bleeding but will decrease the risk of worsening coronary thrombosis.
e. Consider heparin resistance and increase the initial heparin dose to avoid delays in starting CPB because the ACT is too low.
f. Continue antianginal therapy, particularly the nitroglycerin infusion, during an acute myocardial ischemic event.
g. Maintain coronary perfusion pressure. Phenylephrine or norepinephrine boluses and/or infusions may be necessary. An IABP may be in use or required. Maintain IABP triggers.
h. In these cases, time is of the essence. Decisions must be made regarding the risks and benefits of additional monitoring (arterial line and PA catheter) relative to the delay required for catheter insertion. Access to the central circulation and some form of direct blood pressure monitoring are required before surgery can begin.
(1) If all lines are placed before induction at your institution, then the decision involves how to proceed while the patient is awake. If the patient has resolution of chest pain and ECG changes, then proceed cautiously with monitoring line insertion. It is often necessary to replace a femoral PA line with one that is closer to the patient’s head for accessibility. Keep the femoral catheter in place for monitoring until just before floating the new PA catheter, at which time it should be pulled back to avoid complications.
(2) If ischemia is still present while the patient is awake, proceed to the induction of anesthesia with the monitors you have. Often, after anesthesia is induced, the reduction in myocardial O2 demand will significantly improve the ischemia and correct hemodynamic changes. In this case, insertion of further monitoring would be appropriate.
(3) If the patient continues to have significant hemodynamic and ischemic changes, after induction, that are unresponsive to treatment, proceed to CPB urgently.
(4) In an arrest situation, go directly to CPB. The surgeon can hand off central venous and PA lines before weaning the patient from CPB. TEE is a fast alternative to obtain much of the information derived from a PA catheter.
i. Urgency of initiating CPB does not supersede obtaining adequate heparinization documented by ACT, or adequate anesthetic levels. In a cardiac arrest situation, use double or triple the usual dose of heparin to ensure adequate heparinization. The surgeon may give the heparin directly into the heart if access is not available.
j. If a “bailout” (coronary perfusion) catheter has been placed across a coronary dissection, it should not be disturbed. It can be withdrawn from the femoral arterial sheath just before application of the aortic cross-clamp.
k. Fibrinolytic or antiplatelet agents may have been given in the catheterization laboratory. These drugs will increase bleeding before and after CPB.
E. Sternal spread
1. Very high level of stimulation can be expected
2. Visually confirm equal inflation of the lungs after the chest is open.
3. PA catheter malfunction with sternal spread has been reported. Most occurrences are with external jugular or subclavian approaches and involve kinking of the PA catheter as it exits the introducer sheath. A reinforced introducer can decrease the incidence of kinking. The surgeon could decrease the amount of sternal retraction.Sheath withdrawal may rectify the problem but can lead to the following:
a. Loss of the IV line
b. Bleeding
c. Contamination of the access site
4. Innominate vein rupture, as well as brachial plexus injury, is possible after aggressive sternal spread.
F. IMA and radial artery dissection
1. This is a period of low-level stimulation.
2. The chest is retracted to one side using the chest wall retractor, and the table is elevated and rotated away from the surgeon. The left IMA (LIMA) is most commonly grafted to the left anterior descending artery.
a. This procedure can cause difficulties in blood pressure measurement.
(1) Left-sided radial arterial lines may not function during LIMA dissection owing to compression of the left subclavian artery with sternal retraction. The same may be true with a right-sided catheter and a right IMA (RIMA) dissection.
(2) Transducers must be kept level with the right atrium.
b. Extubation may occur with patient movement during retraction.
c. Radial nerve injury due to compression by the support post of the Favaloro retractor is possible.
3. Bleeding may be extensive but hidden from view in the chest cavity (consider volume replacement to treat hypotension).
4. Heparin, 5,000 units, may be given during the vessel dissection process.
5. Papaverine may be injected into the IMA for dilation and to prevent spasm. Systemic effects may include hypotension or anaphylaxis.
6. IMA blood flow usually should be more than 100 mL/min (25 mL collected in 15 s) to be considered acceptable for grafting.
7. Mechanical ventilation may need to be adjusted if the motion of the lungs interferes with the surgical dissection of the IMA. This may be achieved by reducing the tidal volume and increasing the respiratory rate to achieve constant minute ventilation.
8. If the radial artery is being harvested as a conduit, the arterial line should be placed on the other side.
G. Sympathetic nerve dissection
1. After the pericardium is opened, the postganglionic sympathetic nerves are dissected from the aorta to allow insertion of the aortic cannula.
2. This is the most overlooked period of high-level stimulation because of sympathetic discharge. Treatment of hemodynamic changes is explained in Section I.C.
II. Perioperative stress response
A. Afferent loop
1. The body responds to stress with a catabolic response and an increase in substrate mobilization. This response is mediated primarily through the hypothalamic–pituitary–adrenal axis.
2. Stimuli that can trigger this response include the following:
a. Psychologic
(1) Preoperative anxiety
(2) Light anesthesia, awareness
b. Physiologic
(1) Pain associated with invasive monitor placement
(2) Intubation
(3) Surgical stimulation
(4) Changes in blood pressure (hypotension or hypertension)
(5) Hypoxia
(6) Hypercapnia
(7) CPB
(8) Aortic cross-clamp removal
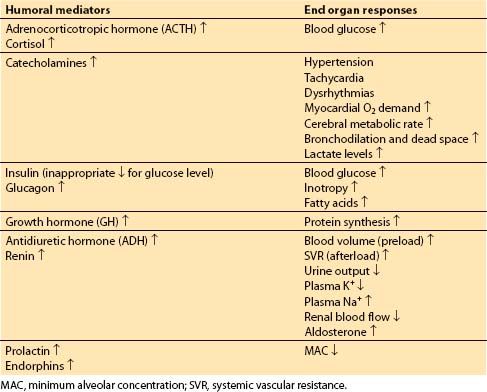
B. Humoral mediators and the systemic effects of the stress response: (see Table 7.2)
Table 7.2 Stress response—mediators and systemic response







Full access? Get Clinical Tree


