Fig. 21.1
(a, b) The AUB clock Tower before and after destruction. (c) Center of Beirut destroyed
Statistics
Between April 1975 and November 1976, 8,324 casualties came though the Emergency Room of AUB (Table 21.1). The age range was newborn to 76 years but most were adult males 14–30 years; only 20 % were >30 years and 10 % <14 years. Gender differences were males 87 %, and females 13 %. Shrapnel was the cause of injury in 66 %, bullet wounds in 29 %, and blast injuries and extensive burns in 5 % [2]. Abdominal injuries were most common at 35 %, followed by chest 21 %, extremities 20 %, head 13 %, spine 2 %, mandible 1 %, and multiple injuries 8 % (Table 21.2).
Table 21.1
Casualties received at the American University of Beirut Medical Center from April 1975 to November 1976
Month | Casualties treated in E.R. | Total deaths | Admitted to AUBMC from ER | Deaths in OR |
|---|---|---|---|---|
1975 | ||||
April | 60 | 1 | 24 | 0 |
May | 38 | 7 | 9 | 1 |
June | 28 | 0 | 12 | 0 |
July | 41 | 1 | 24 | 0 |
Aug. | 10 | 1 | 0 | 1 |
Sept | 86 | 0 | 31 | 0 |
Oct. | 110 | 1 | 58 | 1 |
Nov. | 73 | 4 | 32 | 2 |
Dec. | 235 | 5 | 58 | 1 |
1976 | ||||
Jan. | 375 | 10 | 149 | 3 |
Feb. | 92 | 4 | 25 | 2 |
Mar. | 788 | 39 | 207 | 3 |
Apr. | 609 | 22 | 135 | 9 |
May | 1,114 | 76 | 243 | 12 |
June | 1,131 | 49 | 245 | 7 |
July | 793 | 52 | 132 | 1 |
Aug. | 1,008 | 53 | 143 | 3 |
Sept. | 631 | 33 | 92 | 2 |
Oct. | 750 | 54 | 126 | 6 |
Nov. | 352 | 17 | 57 | 0 |
8,324 | 429 | 1,802 | 54 | |
5.15 % | 2.99 % | |||
Table 21.2
Statistical analysis of operated casualties according to their sex, age, cause, and site of injury
Sex | Male 87 % | Female 13 % |
Age | 70 % 14–30 years | |
20 % more than 30 years | ||
10 % less than 14 years | ||
Cause of injury | Shrapnels 66 % | |
Bullets 66 % | ||
Blast 5 % | ||
Site of injuries | Abdominal injuries | 35 % |
Chest | 21 % | |
Extremities | 20 % | |
Head | 13 % | |
Spine | 2 % | |
Mandibular | 1 % | |
Multiple | 8 % | |
Anesthesia | Ketamine induction | 55 % |
Thiopentone induction | 40 % | |
Regional anesthesia | 3 % | |
No anesthesia | 2 % | |
Blood transfusion | 50 % received blood transfusion | |
Intraoperative death | 2.9 |
Dead on Arrival
Patients dead on arrival at the Emergency Room had usually succumbed immediately from overwhelming injury or from exsanguination (Fig. 21.2a–c) Death from trauma occurs in a trimodal fashion. Fifty percent of deaths in the theater of war are immediate and result from massive injury to a major vessel, the heart, the brain, or the spinal cord. After a hiatus period, sometimes called the “golden hour,” 30 % of deaths occur as a result of potentially treatable conditions such as hypoventilation, hemorrhage, hemopneumothorax, cardiac tamponade, or an expanding intracranial mass. Days to weeks later, 20 % of patients die from sepsis or multiple-organ failure, or both.

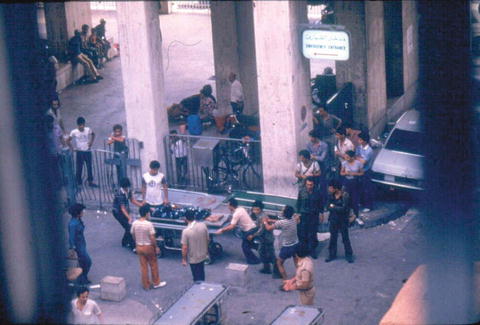
Fig. 21.2
(a, b) Death on arrival. (c) Death in the operating room
Triage
Triage in the emergency room (Fig. 21.3) consisted of assigning patients to one of the three categories:
1.
Seriously injured patients were stabilized using measures such as fluid resuscitation, endotracheal intubation, and ventilation. They were then transferred for further investigation or surgery, or sent to the recovery room.
2.
Patients with lesser injuries were taken to the outpatient department reception area, where interns and medical students managed minor problems. Patients were then discharged home.
3.
Patients who were dead on arrival were transferred to the morgue.
Fig. 21.3
Emergency room during an attack
Challenges of Anesthesia
Table 21.3 illustrates some of our challenges. Unprepared for such a massive onslaught personnel were afraid. Also, given the large exodus of many who were able to leave Lebanon, we were short not just of supplies but also of skilled people.
Table 21.3
Statistical analysis of operated casualties according to their sex, age, cause, and site of injury
1. Problems related to the civil war itself |
2. Personnel deficiency (death, exodus, isolation, and nervous exhaustion) |
3. Deficiency of supplies particularly oxygen and nitrous oxide |
4. Work load |
5. Problems of anaesthesia of the seriously traumatized patients such as (a) respiratory failure (b) shock, cardiac tamponade, flail chest… (c) full stomach |
6. Special problems (a) postoperative respiratory failure (b) tetanus (c) gas gangrene (d) decompression sickness |
Oxygen and nitrous oxide were in shortest supply. We economized gas by using low flows via a carbon dioxide absorption circuit. All respirators driven by oxygen (Ohio, Bird, etc.) were retired. Finally we used compressors to feed room air into anesthesia machines. The noise of these machines compelled us to turn to simple draw over equipment such as the Epstein, Mackintosh, and Oxford (EMO) inhaler (Fig. 21.4a, b).
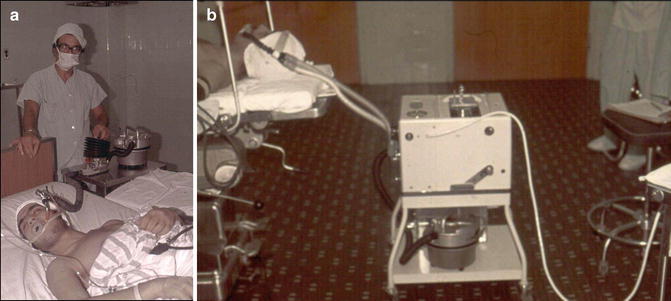
Fig. 21.4
(a, b) Patient anesthetized with ether using the EMO inhaler. The EMO inhaler connected to the Radcliffe respirator
Preoperative Assessment
As many as 150 casualties might come in simultaneously and we had to transfer more severely injured cases to the recovery room where they were assessed, resuscitated and triaged further (Fig. 21.5). Cardiac tamponade and major vessel injuries were given first priority. Life-threatening trauma cases were transferred directly to the operating room which was in close proximity to the recovery room. Table 21.4 lists our assessment.

 The Evolution of Surgical Humanitarian Missions
Management of Pain in Less Developed Countries
Trauma, War, and Managing Vascular and Orthopedic Injuries
The Evolution of Surgical Humanitarian Missions
Management of Pain in Less Developed Countries
Trauma, War, and Managing Vascular and Orthopedic Injuries
 What Do Patients and Communities Expect of a Medical Mission?
What Do Patients and Communities Expect of a Medical Mission?
 Legal and Ethical Issues in Global Health: A Trip Through the Vagaries of Truth and Culture
Legal and Ethical Issues in Global Health: A Trip Through the Vagaries of Truth and Culture
 Anesthesiologists’ Role in Disaster Management
Anesthesiologists’ Role in Disaster Management



Related posts:
The Evolution of Surgical Humanitarian Missions
Management of Pain in Less Developed Countries
Trauma, War, and Managing Vascular and Orthopedic Injuries
What Do Patients and Communities Expect of a Medical Mission?
Legal and Ethical Issues in Global Health: A Trip Through the Vagaries of Truth and Culture
Anesthesiologists’ Role in Disaster Management
Full access? Get Clinical Tree
