Fig. 18.1
Flexile screen placed at the head of the table serves to protect the face, enable communication with the patient, and to monitor the airway
The anesthesiologist will need to assess the patient after positioning to further plan for management of the airway by inserting a laryngeal mask airway (LMA) or direct laryngoscopy using a flexible fiberscope should the clinical situation arise. In some situations, the use of a nasal airway placed under topical anesthesia may be used to prevent soft tissue obstruction throughout the operation. Some anesthesiologists prefer to manage the airway differently and elect to place an LMA or a nasal endotracheal tube under local anesthesia from the start.
Monitoring
As in general anesthesia , standard monitoring includes electrocardiogram , blood pressure and respiratory rate, end-expiratory CO2, pulse oximetry, urine output, and a monitor to assess the depth of sedation (see Chap. 11, “Clinical Application of Raw and Processed EEG”). Monitoring by direct observation offers valuable information regarding the patient’s comfort level, specialized neurologic testing, and fosters trust and allays anxiety.
Throughout the procedure, oxygen is delivered to the patient by nasal cannula or by face mask. Both of these devices should be attached to a line for continuous monitoring of end-expiratory CO2 and the respiratory rate. Monitoring the respiratory rate will guide the administration of opioids. Should the decision be made to insert an arterial line, it should be done very gently under local anesthesia or under deep sedation in the asleep–awake–asleep technique (see further discussion). Use of an arterial line minimizes discomfort from the frequent inflation of the blood pressure cuff, provides continuous blood pressure measurement, and facilitates sampling for arterial blood gases and other values. Some centers use a simple processed electroencephalogram (EEG) to guide the administration of propofol and other sedatives.
Sedation and Analgesia
Sedative and analgesic medications are generally used in preparation for surgery and during the first and third stages of the procedure [12–15]. A variety of agents may be used for sedation and analgesia. Midazolam is useful as a premedication while short-acting agents that are more easily titrated are used during surgery. Midazolam is frequently avoided if electrocorticography is planned for seizure mapping or in older patients who may not be able to cooperate during testing.
Propofol is the agent most used for sedation during surgery as it is a short-acting drug that has a fast onset of action and a short recovery period [15–18]. At low concentrations, propofol has the added advantage of antiemetic effects by its action on the cannabinoid receptors [19]. The administration of propofol may be guided by the use of continuous monitoring of the processed EEG [16, 17]. Opioids may be administered during surgery to supplement analgesia in the event that there is discomfort from a patchy regional block, positioning, or the urinary catheter. A variety of opioids may be administered either as bolus injections or by infusion. A fast-acting opioid with a short half-life and rapid recovery such as remifentanil has all of these advantages [20] and is our opioid of choice. In our practice, we start remifentanil at 0.1 μg/kg/min and adjust the infusion rate to keep respiratory rate between 8 and 12 breaths per minute before starting a low-dose propofol, which is usually less than 25 μg/kg/min. It is not unusual for some patients to require a higher dose of remifentanil, up to 0.18 μg/kg/min, while some other patients may require a lesser dose. Therefore, it is essential to monitor respiratory rate and reach the proper remifentanil infused dose before the start of the propofol infusion. The use of optimal narcotic dose helps the patient to tolerate surgical position and discomfort of the urinary catheter. Others use higher doses of propofol and lower remifentanil. It is important to have propofol and remifentanil infusions enter the intravenous line at the catheter or to use dedicated intravenous lines to prevent inadvertent bolus injections.
Dexmedetomidine is a selective alpha-2 adrenergic agonist that works on the subcortical level (locus ceruleus) and has been used to provide sedation and some analgesia without respiratory depression; however, it has no amnesia [21]. Dexmedetomidine acts at the brainstem and in many parts of the body, including the smooth muscles of the blood vessels, thus explaining why higher doses can result in bradycardia and hypotension. Dexmedetomidine has a rapid onset, is metabolized by the liver, and excreted by the kidney. Dexmedetomidine has a distribution half-life of 6 min and a clearance half-life of 2 h, which is longer than propofol . It was first used in functional neurosurgery by Bekker et al. [22] and its use has been supported by others [23, 24]. Typical doses of dexmedetomidine used to achieve the desired level of sedation and analgesia range between 0.2 and 0.6 μg/kg/h administered by continuous infusion [25].
Regional Anesthesia
Regional anesthetic blocks of nerves innervating the scalp are superior to local infiltration to blunt the responses to Mayfield pin placement and surgical stimulation, and to provide postoperative pain control [26–28]. A variety of local anesthetic agents may be used for the regional anesthesia. Long-acting agents with minimal side effects in combination with epinephrine in a final concentration 1:200,000 are often used. The goal is to achieve a block that lasts for the duration of the procedure and afterward to afford postoperative pain relief.
The scalp is innervated, on each side, by six nerves (Fig. 18.2), four of which are branches of the trigeminal nerve and two originate in the cervical region. The four branches of the trigeminal nerve are the Supratrochlear, Supraorbital, Zygomaticotemporal, and Auriculotemporal. The lesser and greater occipital nerves originate from branches of the second and third cervical nerve roots [2, 26, 29–31]. These nerves may be blocked individually or captured in a continuous ring. Individual blocks have longer duration and require the use of less medication and thus lower the risk of possible side effects. The details of regional anesthesia of the scalp are presented in Table 18.1. All injections are done after negative aspiration.
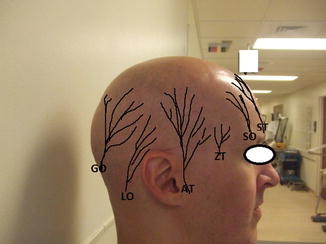
Fig. 18.2
Picture of the head shows drawing of the six nerves that innervate the scalp . GO is greater occipital nerve, LO is lesser occipital nerve, AT is auriculotemporal nerve, ZT is zygomaticotemporal nerve, SO is supra orbital nerve, and ST is supratrochlear nerve
Table 18.1
Regional anesthesia of the scalp, doses used at Northwestern University
Supratrochlear branch | Blocked at the supratrochlear notch, which easily can be palpated where the bridge of the nose meets the supraorbital ridge. The direction of the short 25G needle should be perpendicular to the notch to prevent the needle from sliding down into the orbit or up toward the forehead (Video 18.1) | 1 mL |
Video 18.1–ST | ||
Supraorbital branch | Blocked at the supraorbital notch in the middle of the upper eyebrow usually in direct line with the pupil of the eye. The short 25G needle should be directly perpendicular to the notch to prevent the needle from sliding down into the orbit or up toward the forehead (Video 18.2) | 1 mL |
Video 18.2-SO | ||
Zygomaticotemporal branch | Blocked at a point just above the zygomatic arch lateral to midway between the orbital edge and the tragus of the ear | 3–5 mL |
Video 18.3-ZT | The 25G needle, 38 mm long, is inserted to the surface of the temporal bone and slides forward toward the orbit. After negative aspiration, 3 mL local anesthetic injected, the needle withdrawn one cm then 1 cm3 anesthetic injected. Again the needle withdrawn 1 cm followed by the injection of 1 cm3 more of local anesthetics. This is performed at the side of surgery. The nonsurgical side, only 3 cm3 are injected | |
Auriculotemporal branch | Blocked 1 cm above the tragus just posterior to the superficial temporal artery. This modification is to avoid possible facial nerve palsy [32] | 3 mL |
Video 18.4-AT | ||
Lesser occipital nerves | The lesser occipital nerve is blocked by the injection of local anesthetics in the grove palpated just behind the mastoid at straight line behind the tragus (video 18.2). An alternative method is to perform the block at 2.5 cm lateral to the greater occipital nerve block along the superior nuchal line | 3 mL |
Video 18.5–LO | ||
Greater occipital nerves | Blocked at the superior nuchal line just medial to the occipital artery or one-third of the distance along a line drawn from the greater occipital protuberance and the mastoid | 3 mL |
Video 18.6-GO |
The choice of local anesthetic for the scalp blocks should be one with a rapid onset and a long duration. Many agents may be used including bupivacaine, lidocaine, ropivacaine, levobupivacaine, and tetracaine. Epinephrine in a final concentration of 1:200,000 may be used in conjunction with these agents to prolong the duration of the block. Our current practice at Northwestern University incorporates the use of 6 mL of tetracaine 1 % (60 mg) mixed with 30 mL of 1 % lidocaine with epinephrine 1:200,000 (300 mg). We perform bilateral blocks of the six nerves. The total volume injected of this mixture, lidocaine/tetracaine , is 30 mL, which contains 50 mg tetracaine and 250 mg lidocaine. This technique reliably enables us to immediately place the three pins head holder comfortably. Also, it is associated with stable vital signs, provides 8 h of surgical time, and up to 22 h of pain relief. In 9 years, we have had no side effects or local anesthetic toxicity to report. In most cases, regional anesthesia of the scalp provides sufficient surgical anesthesia for the duration of the surgery. Should a patient experience pain after the craniotomy while mapping, the scalp blocks may be supplemented with a dural block as described in the following section.
A faster, though less specific approach to anesthesia of the scalp is provided by infiltrating in a line that essentially connects the injection sites of the six branches at their roots in addition to infiltrating the surgical incision site with a field block. This approach leads to a less solid block and is associated with the use of higher doses of local anesthetic.
Anesthetic Management
The anesthetic management for neurosurgical procedures in patients that are awake may be divided into at least three categories. The first may be termed Asleep Awake Asleep (AAA). Variations of this technique are used by many anesthesiologists [15, 23, 31–36]. In the early stages of the procedure including provision of anesthesia for the scalp, Mayfield pin insertion, skin incision, craniotomy, and provision of anesthesia of the dura, general anesthesia is provided to assure patient comfort. The patient is anesthetized with a combination of short-acting agents such as propofol, or dexmedetomidine and an ultra-short-acting opioid. Airway management may be augmented by insertion of an LMA or a nasal endotracheal tube. The nasal endotracheal tube is placed into the trachea in the initial or “Asleep” stage, withdrawn to the level of the pharynx in the second or “Awake” stage, and reintroduced back to the trachea during the final “Asleep ” stage. The anesthetic technique preferred at the second author’s institution, is deep sedation with a nasal endotracheal tube positioned in the posterior pharynx under fiber optic control, which remains in place throughout surgery. This ensures safe airway management with spontaneous ventilation during the craniotomy and allows a smooth transition to an awake patient who is able to participate and speak without airway irritation. It also provides a mechanism for a safe and efficient endotracheal intubation if warranted during closure or at any point in case of emergency.
When an LMA is utilized, it is positioned around the vocal cords during the first and last stages of the surgery. The disadvantages of this technique are the potential for irritation of the airway during endotracheal tube or LMA manipulation, and for paradoxical responses to the anesthetics administered during the intermediate “Awake” stage. Another potential problem is that of movement of the head during the transitions between anesthetic depths with the risk of patient injury.
In the AAA technique , during the “awake” phase, the surgeon may need to anesthetize the dura before incising it. If needed, a short-acting anesthetic agent such as mepivacaine or lidocaine would suffice for the roughly 2 h needed for brain mapping and tumor resection in the awake patient. Dural anesthesia may be achieved during the transition from sedation after the craniotomy has been completed in one of two ways: the meningeal trigeminal branches may be blocked by injecting a local anesthetic into the base of the projected dural flap with a fine (25–30 gauge) needle. In elderly patients or others in which the dura is very thin, this procedure carries a risk of damaging cortical vessels and causing a subdural hematoma. In our experience (Bonn University), a very effective method uses anesthetic-soaked cottonoids or compresses applied to cover the dural flap for 5 min before incision, and on the base of the dural flap until closure. For example, 10–20 mL of 1 % mepivacaine is sufficient for a large craniotomy. This application technique provides rapid anesthesia to the dura, does not interfere with the progress of the procedure, and contributes little to the total volume of local anesthetic with regards to the risk of systemic local anesthetic toxicity.
Another anesthetic management technique, and the preferred method at the first author’s institution, is one that provides sedation along a spectrum of different depths while maintaining the patient in an awake or readily arousal state. This is commonly referred to as monitored anesthesia care (MAC) with sedation. In this technique, we use remifentanil at higher doses (0.05–0.18 μg/kg/min) to maintain a respiratory rate of 8–12 in addition to a small infusion of propofol, which is usually less than 25 μg/kg/min. The patient will be awake at all times with varying degrees of sedation and analgesia to maintain good ventilation, oxygenation, and a clear airway.
Recently, the complete awake–awake–awake technique without sedation has been advocated by Hansen et al. [11]. In this technique, medication is substituted by psychologic intervention.
Cortical and Subcortical Mapping and Neurologic Monitoring
Surgery performed on a patient who is awake and cooperative allows for testing of all neurologic functions. The utility of the technique is limited, however, by the total duration of the procedure , the patient’s position, and the operative setting. Completion of the procedure in less than 2 h is optimal as the patient’s position may be difficult to tolerate for extended periods of time. During an awake procedure performed with continuous sedation, the patient often tolerates longer periods of operative time.
The specific test of neurologic function is dependent on the location of the target lesion. Motor function may be difficult to monitor clinically. However, motor and sensory function can be assessed in the anesthetized patient with neurophysiologic methods. Cognitive functions such as language, calculation, spatial orientation, memory, and even emotion may also be tested under awake conditions. However, there are no established intraoperative protocols for these assessments. Typically, surgery in an awake patient is all but required for language preservation in the face of lesions of the left or dominant hemisphere.
Language testing requires some linguistic expertise and is frequently performed by a dedicated psychologist or linguist. Apart from specific expertise in language testing, reassurance and support for the patient undergoing a craniotomy while awake is a key factor for successful mapping and monitoring. An experienced anesthesiologist with interest in and familiarity with these procedures may perform the testing. There is broad consensus among groups performing awake surgery that a naming paradigm is suited to map and monitor the essential aspects of language function [37]. A picture of an object is presented for 4 s and is named by the patient, often embedded into a carrier sentence such as “This is a banana.” During this time, the surgeon does or does not stimulate the cortex or the subcortical fibers.
Neurologic testing comprises both mapping and monitoring. Using the example of language production, mapping refers to the identification and delineation of eloquent cortical areas and subcortical fiber tracts, which are involved in preserving these structures during lesion resection. Monitoring refers to continuous or intermittent testing of some target function in order to detect and avert functional impairment due to ischemia or other insult. These are complementary aspects of intraoperative functional preservation. Mapping requires electrical stimulation of the cortex or the white matter in order to elicit or, more frequently, inhibit a neurologic function. In these cases, the patient may perceive a “tugging” or motor movement that is not perceptible to the observant anesthesiologist.
Cortical areas where reproducible speech inhibition by stimulation is encountered, are defined as essential for language production. However, there is no reproducible evidence to date that proves that all of these areas are truly indispensable. Typically, bipolar electrical stimulation at a frequency of 50–60 Hz for 1–4 s is employed (Ojemann stimulator). However, stimulation using a high-frequency stimulator, similar to that used for transcranial motor evoked potential stimulation, can be used and is associated with a lower incidence of induced seizures [37–39]. The stimulation parameters are discussed by Szelenyi et al. [40]. It is important to avoid the induction of clinical or subclinical seizures from excessive cortical stimulation [41]. Ideally, the stimulation threshold for after discharges (as a prestage of seizure) is determined by electrocorticography (ECoG) recordings from strip electrodes positioned around the target area, prior to the actual mapping procedure.
Induction of clinical or subclinical focal seizures is rarely dangerous. However, such activity can distort the mapping results, prompting the need for intervention. Irrigating the surgical field with cold Lactated Ringers solution is usually sufficient to interrupt the seizure activity [42]. Sedative drugs such as benzodiazepines should be avoided in order to preserve the patient’s wakefulness and cooperation for further testing. However, a small dose of propofol (25–50 mg) may be needed if cold irrigation is inadequate. Secondary generalization of seizures hardly ever occurs and can be handled as indicated in the next paragraph.
Complications
Craniotomies, whether they are performed under general, MAC, or AAA anesthesia, are associated with the same complications [2, 31]. As cited, seizures may occur as a result of stimulation during neurologic testing or from excessive use of local anesthetics. Depression of ventilation due to heavy sedation or opioid use may lead to hypercarbia and/or hypoxemia. This may be minimized by careful monitoring and the use of short-acting agents in dedicated intravenous lines. Nausea and vomiting are troublesome intraoperative issues for awake patients and may be minimized by pretreatment with antiemetic medications and the use of low doses of propofol infusion. Nausea related to surgical maneuvers and direct dural irritation may be difficult to prevent and treat pharmacologically and may be relieved only by decreasing surgical stimulation. The ambient room temperature should be adjusted to the liking of the patient and intravenous fluids should be warmed to prevent and minimize shivering. If shivering occurs despite these other maneuvers, it may be effectively treated with medication such as small doses of meperidine, clonidine, or physostigmine. Hemodynamic changes such as hypertension may occur and can be easily treated with beta-blockers and medication to ease anxiety. Pain as a result of poor local anesthesia may occur and should be supplemented by analgesic agents and additional infiltration of local anesthetics, if appropriate. The possibility of local anesthetic toxicity should be kept in mind and the total dose of infiltrated local anesthetics should be calculated and tracked including local anesthetics used during the insertion of the Foley catheter. At times, sedation may yield a paradoxical effect and lead to disinhibition and a lack of cooperation. In this case, the infusion of a sedative or analgesic medication may be decreased or stopped until the patient returns to an appropriate baseline or may require pharmacologic reversal. Seizures may occur during neurologic testing and can be treated as described in the previous section. Significant blood loss may be a complication. The incidence of air embolism is actually increased during awake craniotomies due to the negative intrathoracic pressure, with coughing being the first sign.
Complications related to performing the scalp blocks, such as nerve injury, intravenous and intra-arterial injection, intracranial injection, infection, and facial nerve palsy can occur [43]. To minimize such complications, we modified the auriculotemporal block by performing the block 1 cm above the tragus just behind the superficial artery and decreasing the volume from 5 to 3 mL [32].
Anesthesia for Awake Neurovascular Procedures
Anesthesia for Awake Deep Brain Stimulation
Deep brain stimulation (DBS) is a specific procedure performed in an awake patient. The procedure is performed using a stereotactic technique and has proved beneficial in the treatment of central movement disorders, epilepsy, psychiatric disorders, and obesity [47, 48]. In the case of Parkinson’s disease, it has emerged as a therapeutic modality [49–51].
If a deep brain electrode is to be placed on only one side of the brain, then it should be mentioned that clinical motor testing will be conducted on the contralateral upper extremity. For this reason, the intravenous line, arterial line (frequently used to monitor hypertension), and noninvasive blood pressure cuff should all be placed on the ipsilateral arm to avoid interfering with the clinical testing. In the anesthetic management for DBS, infusions of short-acting agents may be used (e.g., propofol, remifentanil). And these agents are avoided during single unit acquisition. Medication administration should be stopped in time to allow recovery before actual neurologic testing so that the nucleus may be identified [52]. Gamma-aminobutyric acid (GABA) receptor-mediated medication (e.g., benzodiazepines) should be avoided because they may inhibit the tremor, which is the endpoint of awake testing. Most anesthetics that act on GABA receptors interfere with the DBS testing and should be used with care [53]. Even ultra-short-acting agents such as propofol and remifentanil should be stopped intraoperatively in time for testing as both agents have been reported to interfere with accurate results [54]. Certain medications may interfere with the neurologic testing and should not be administered during DBS procedures such as phenothiazine, droperidol, and metoclopramide [55, 56]. The α-2 receptor agonist and to a lesser degree the μ-opioid receptor agonist dexmedetomidine can be used as it has no effect on the microelectrode recording (MER) testing. Frequently encountered, intraoperative hypertension must be aggressively treated to avoid intracranial bleeding (often below 140 mmHg) and hydralazine and infusions of sodium nitroprusside, nitroglycerine, or nicardipine are used (beta-blocking agents are avoided since they may reduce the tremor activity).
Unwanted side effects to the insertion of DBS electrodes may include motor phenomena such as muscle contractions or dysphasia from stimulating the corticospinal or corticobulbar efferent of the internal capsule. In such cases, electrodes are repositioned. Others may include sensory perceptions including transient paresthesia or visual flashes. (For more information on DBS testing and monitoring, see Chap. 5, “Deep Brain Stimulation.”)
Certain complications may occur during DBS procedures. These include respiratory depression, airway obstruction, hypoxemia, nausea, vomiting, seizures, hypertension, sneezing, bronchospasm, pulmonary edema, angina, and air embolism [53, 57]. Some complications may occur in the postoperative period, such as bleeding, seizures, or a neurologic deficit [57]. In general, there is no one anesthesia protocol, but a variety of methods, often influenced by personal experiences, that are not necessarily supported by solid literature.
Related posts:







Full access? Get Clinical Tree


