Anatomy of the Brachial Plexus
Laura Clark
Knowledge of anatomy is essential to maximize the likelihood of success when performing peripheral nerve blocks. However, it is important to recognize that variations are frequent, and that “normal anatomy” is only found in 50% to 70% of cases.
Brachial Plexus Anatomy (FIG. 6-1)
The brachial plexus is formed by the anterior rami of C5 to T1 (the posterior roots give innervation for skin and muscle of the paravertebral area). Brachial plexus innervates the scapular belt and the upper limb. It has a triangular shape with the base applied against the cervical spine and the vertex in the axilla. The anterior rami supply the superior (C5-6), middle (C7), and inferior (C8-T1) trunks. At the level of the superior border of the first rib, each trunk divides into an anterior and posterior division. The three posterior divisions join to form the posterior cord. At the level of coracoid process, the anterosuperior and middle divisions form the lateral cord and the anteroinferior division becomes the medial cord. The axillary and radial nerves originate from the posterior cord. The musculocutaneous nerve quickly separates from the main brachial plexus as it passes underneath the clavicle and becomes a single nerve as the plexus transitions from divisions to cords. In the vertex of the axilla, the lateral cord and part of the medial cord join to form the median nerve; the medial cutaneous nerve of the arm and the forearm and finally the ulnar nerve originate from the remainder of the medial cord. See Figure 6-1 for the classical two dimensional picture of the brachial plexus highly recommended to review the anatomy in a fresh tissue cadaver whenever possible. In Figures 6-2 and 6-3 minimal alteration of the anatomy in these fresh tissue dissections demonstrate the brachial plexus and the surrounding anatomy in situ.
Embryology allows us to better understand the apparent complexity of the brachial plexus. During organogenesis, between the 4th and the 8th week of development, the brachial plexus has a cone shape in the bud limb. The cutaneous innervation is distributed at the periphery of the trunk wall. As the bud limb grows, dermatoma stretches out. The cone then divides longitudinally into two independent plans, anterior and posterior, with the appearance of three cords. The posterior cord (posterior plane) provides innervation to the extensor and supinator muscles while the anterior plane, more complex and variable, provides the medial and lateral cords that innervate the flexor and pronator muscles. Generally there is no anastomosis between the anterior and posterior cords. The presence of the subclavian artery explains why there are two anterior cords. Thus, in some species without the subclavian
artery (birds) only one anterior cord is found. Embryogenesis also explains the frequency of variations and anastomosis between the nerves originating from the anterior cords.
artery (birds) only one anterior cord is found. Embryogenesis also explains the frequency of variations and anastomosis between the nerves originating from the anterior cords.
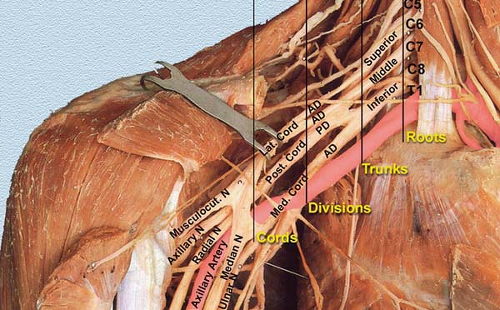 Figure 6-1. Brachial plexus anatomy. |
Usually the anterior rami of C4 and T2 also contribute to the brachial plexus. This contribution allows one to differentiate a “prefixed” plexus with a C4 predominant contribution versus a “postfixed” plexus with a T2 predominant contribution. In humans, the brachial plexus is predominantly “prefixed.” This differentiation may explain the superior extension toward C4 that frequently occurs after an interscalene block (prefixed).
Nerve Courses
Collateral Branches
Twelve branches originate from the brachial plexus. Some are more relevant than others when performing brachial plexus blocks. They include:
The long thoracic nerve that directly originates from the C5 to C7 roots. It supplies the serratus anterior muscle. The nerve runs posterior to the brachial plexus. Therefore, when performing an interscalene block, the stimulation of the serratus anterior muscle suggests that the needle should be redirected anteriorly.
The dorsal scapular nerve supplies the levator scapulae and rhomboid minor and the superior part of the rhomboid major muscles. It is one of the first nerves to leave the plexus. The stimulation of this nerve produces an elevation of the scapulae (interscalene approach). The injection of local anesthetic solution following its stimulation produces a block of the deep cervical plexus, which may be of interest in the case of a carotid surgery.
The suprascapular nerve supplies both the supraspinatus and the infraspinatus muscles and sends branches to the shoulder joints. It originates at the level of the interscalene groove. Moreover, like the long thoracic nerve, the suprascapular nerve runs posterior to the brachial plexus. Its stimulation, which produces a posterior contraction of the rotator cuff (shoulder ascension), indicates that the needle needs to be redirected anteriorly. Diffusion of local anesthetic toward this nerve after a supraclavicular approach is inconsistent.
The subclavius nerve supplies the subclavius muscle and anastomoses with the phrenic nerve, a nerve that also originates from C5. This explains in part why, even with limited extension to the cervical plexus or limited volume of local anesthetic, a blockade of the phrenic nerve with an interscalene block results in a reversible diaphragmatic paralysis.
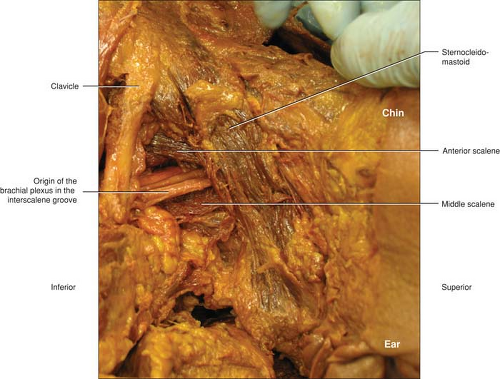 Figure 6-2. A very limited dissection demonstrating how the brachial plexus lies in the neck as transverse from its origin of individual roots from the cervical spine to somewhat join into divisions and group into cords. The divisions travel in a similar plane at this level and are organized in a parallel fashion to each other. The plexus is framed by the sternocleidomastoid at the superior edge of the triangle until it gives way to the anterior border of the anterior scalene. At times the anterior scalene is not prominent as in this specimen. The inferior border is the clavicle. The triangle is completed by the posterior border in the middle scalene muscle. |
Terminal Branches (Anterior Plan) (Fig. 6-4)
Median Nerve
The median nerve is formed in the axilla by the union of the lateral and medial cords. It runs first laterally to the axillary artery and progressively crosses over the brachial artery to become medial to the brachial artery at the inferior third of the arm. It does not give any branch until the inferior part of the arm, although in one-third of cases it provides an anastomosis to the musculocutaneous nerve. Around the elbow several branches originate from the median nerve (articular to the elbow, muscular to pronator teres muscle). About 2 or 3 cm below the elbow, the median nerve provides the interosseous nerve, which innervates the anterior aspect of the flexor digitorum profundus and anterior aspect of the carpal joint, with frequent anastomosis with the posterior interosseous nerve. In the forearm the median nerve runs between the flexor digitorum superficialis and flexor digitorum profundus muscles. At the distal third of the forearm the median nerve runs between the tendons of the flexor carpi radialis and palmaris longus muscle. It is of interest to note that the palmaris longus muscle is absent in 15% of the population. Several centimeters above the wrist crease the median nerve provides a sensory
palmar branch. Finally, the median nerve enters the hand through the carpal tunnel under the flexor retinaculum and divides into small muscular branches innervating a part of the thenar muscles and branches contributing to the palmar digital nerve.
palmar branch. Finally, the median nerve enters the hand through the carpal tunnel under the flexor retinaculum and divides into small muscular branches innervating a part of the thenar muscles and branches contributing to the palmar digital nerve.
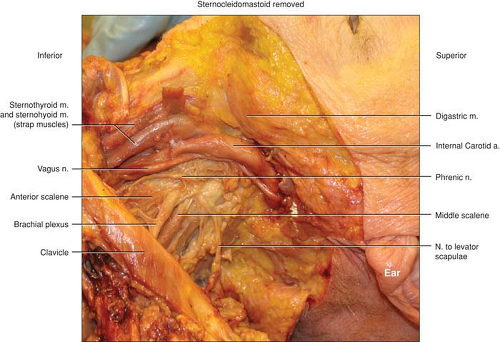 Figure 6-3. The brachial plexus and its surrounding structures. In this dissection the sternocleidomastoid and the internal jugular vein have been reflected away so that the surrounding structures could be better visualized. The close proximity to the phrenic can be appreciated as well as the relatively close internal carotid artery and vagus nerve. Of note in this specimen is an example of how small in diameter the phrenic nerve can be and how close. At the upper end of the origin of the brachial plexus they are almost side by side. This is often demonstrated during performance of an interscalene block with just a very small change in needle direction causing a phrenic nerve stimulation of the diaphragm or the desired twitch of stimulation of the brachial plexus. |
Ulnar Nerve
The ulnar nerve is formed in the upper part of the axilla from the medial cord. Initially the ulnar nerve runs medial to the axillary artery and progressively posterior, reaching the elbow between the medial humeral epicondyle and the olecranon. It leaves its first collateral branch at the elbow for the joint. Below the elbow, branches originate to the flexor carpi ulnaris and part of flexor digitorum profundus muscles. Along the forearm the ulnar nerve runs posterior to the flexor carpi ulnaris and posterior and medial to the ulnar artery. Several centimeters before the wrist crease the ulnar nerve leaves two branches: a palmar branch and a dorsal branch for the palmar and dorsal aspect of the hand. The ulnar nerve enters the hand running under the flexor retinaculum and divides into superficial branches to the palmar digital nerves and deep motor branches that innervate the hypothenar, interosseous, and parts of the lumbrical and thenar muscles.
Musculocutaneous Nerve
The musculocutaneous nerve is a branch of the lateral cord. It leaves the vascular/nervous space high in the axilla, diffusing in the direction of the coracobrachialis muscle,
which it perforates. In the arm, it runs in the groove between the biceps and brachialis muscles. It supplies these two muscles and the coracobrachialis muscle. Several variations of the course and distribution of the musculocutaneous nerve may be observed. In 20% of cases, instead of piercing the coracobrachialis muscle it lies against the median nerve for a variable distance along the arm before supplying the three muscles. It pierces the deep fascia just before the elbow and divides in two branches that run on each side of the cephalic vein and become the lateral cutaneous nerve of the forearm. It supplies the skin of the lateral border of the forearm up to the wrist. In some cases it can extend until the thenar region.
which it perforates. In the arm, it runs in the groove between the biceps and brachialis muscles. It supplies these two muscles and the coracobrachialis muscle. Several variations of the course and distribution of the musculocutaneous nerve may be observed. In 20% of cases, instead of piercing the coracobrachialis muscle it lies against the median nerve for a variable distance along the arm before supplying the three muscles. It pierces the deep fascia just before the elbow and divides in two branches that run on each side of the cephalic vein and become the lateral cutaneous nerve of the forearm. It supplies the skin of the lateral border of the forearm up to the wrist. In some cases it can extend until the thenar region.
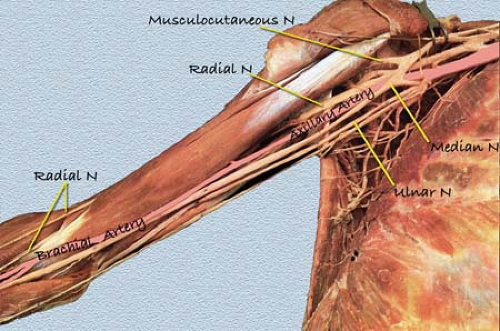 Figure 6-4. Terminal branches (anterior plan). |
Medial Cutaneous Nerve of the Arm and the Forearm
The medial cutaneous nerve of the arm and the forearm are both formed in the medial cord. The medial cutaneous nerve of the arm quickly leaves the plexus in the axilla and dives in the direction of the armpit where it joins the intercostobrachial nerve (Hyrtl anastomosis). It supplies the skin of the medial border of the arm. The cutaneous nerve of the forearm arises from the medial cord and runs with the ulnar nerve until the elbow. In the upper part of the arm it leaves some branches (one or two) for the anterior and internal part of the arm. It pierces the deep fascia just before the elbow and divides in two branches on each side of the basilic vein. It supplies the skin of the medial aspect of the forearm until the wrist.
Terminal Branches (Posterior Plan)
Axillary Nerve
The axillary nerve originates from the posterior cord. It runs deeply against the capsule of the shoulder joint, and it curves posteriorly along the surgical neck of the humerus through a quadrangular space formed laterally and medially by the humerus and the triceps brachii muscle and superior and inferior by the teres minor and major muscles. Then it divides into anterior and posterior branches. It supplies the skin of the inferior half of the shoulder and the lateral aspect of the arm. It also supplies the teres minor and deltoid muscles and gives branches to the shoulder joint.
Radial Nerve
The radial nerve is the extension of the posterior cord in the axilla. It runs initially posterior to the axillary artery and progressively in a spiral course around the humerus in a specific
sulcus to run laterally and then anteriorly at the elbow. It supplies the triceps brachii muscle through a branch leaving at various levels in the axilla. Frequently it leaves a spindly branch to the brachialis muscle. At the third distal part of the arm it leaves branches for the brachioradialis and extensor carpi radialis longus muscles. It supplies skin of the posterior aspect of the arm and the forearm and the lateral border of the elbow. Around the elbow, it gives articular branches to the joint. The cutaneous branch for the forearm leaves the trunk at the inferior part of the radial sulcus. At various levels around the elbow, the radial nerve divides into sensory (superficial) and motor (deep) terminal branches. The superficial branch runs along the lateral border of the forearm and pierces the fascia at the lower third. At this level it is in close relation to the cephalic vein. It supplies the lateral part of skin of the dorsal aspect of the hand. The deep branch (posterior interosseous muscle) winds posteroinferiorly around the neck of the radius and runs between the superficial and deep planes of the extensor muscles. It supplies all extensor and supinator muscles and the dorsal face of the carpal joint.
sulcus to run laterally and then anteriorly at the elbow. It supplies the triceps brachii muscle through a branch leaving at various levels in the axilla. Frequently it leaves a spindly branch to the brachialis muscle. At the third distal part of the arm it leaves branches for the brachioradialis and extensor carpi radialis longus muscles. It supplies skin of the posterior aspect of the arm and the forearm and the lateral border of the elbow. Around the elbow, it gives articular branches to the joint. The cutaneous branch for the forearm leaves the trunk at the inferior part of the radial sulcus. At various levels around the elbow, the radial nerve divides into sensory (superficial) and motor (deep) terminal branches. The superficial branch runs along the lateral border of the forearm and pierces the fascia at the lower third. At this level it is in close relation to the cephalic vein. It supplies the lateral part of skin of the dorsal aspect of the hand. The deep branch (posterior interosseous muscle) winds posteroinferiorly around the neck of the radius and runs between the superficial and deep planes of the extensor muscles. It supplies all extensor and supinator muscles and the dorsal face of the carpal joint.
Related posts:





Full access? Get Clinical Tree


