Fig. 21.1
Exposure of the vessels for renal transplantation in the right iliac fossa. Visualized is the external iliac artery and external iliac vein
It should be noted that the renal graft should be kept cool from the time of cross clamp of the arterial inflow in the donor to reperfusion in the recipient. The kidney is packaged in iced preservation fluid during transport and should be maintained in a similar cool solution during the benching process. Throughout the time of the vascular anastomosis the kidney is packed in ice and wrapped in a cool laparotomy sponge.
Prior to initiation of the vascular anastomosis and reperfusion induction agents should have been started and the patient must be hemodynamically stable. Systemic heparin is usually given to patient approximately 3 min prior to the clamping of the iliac artery and vein. The surgeon then proceeds with complete vascular clamping of the external iliac artery and vein. The venous anastomosis is usually completed first. A venotomy is fashioned with an #11 blade and then extended using Potts scissors. The graft renal vein to recipient external iliac vein anastomosis is then completed in a running fashion with 5-0 or 6-0 synthetic, permanent, monofilament suture (Prolene). Care is taken to avoid purse string narrowing of the anastomosis and/or back wall narrowing. If a graft extension is required and no donor vena cava is attached (as is the case with all L kidneys), stored cadaveric vein can be used. Synthetic graft is not recommended due to the very high thrombosis rate.
Next the arterial anastomosis is performed. This is done after vascular clamps are placed on the proximal and distal external iliac artery. After a small arteriotomy is made, it is extended using Potts scissors or a 4 or 6 mm cardiac punch. The anastomosis is done in a running or an interrupted fashion with 5-0 or 6-0 synthetic, permanent, monofilament suture (Prolene). Several options exist with multiple arteries including separate implants on the external iliac artery, creating a common patch prior to implantation.
The time for completion of the arterial and venous anastomosis is approximately 30–50 min depending on the complexity on the anastomosis. Prior to vascular clamp removal and reperfusion of the graft, the patient is usually given a diuretic (Lasix and/or mannitol) and assessment of appropriate volume status and systolic blood pressure. Clamps are then carefully removed, venous followed by arterial. The renal graft then will quickly regain turgor and a pink color. Deliberate and quick assessment of the renal anastomoses and hilum is undertaken to assess and repair suture line or hilar open vessel bleeding and investigate for thrombosis. This is the most likely time that surgeons will encounter brisk bleeding. In the event that there is thrombosis or uncontrollable bleeding, the option of reclamping the vessels and removing the graft and flushing on the back table does exist.
After the kidney has demonstrated good perfusion, hemostasis has been maintained, and the patient is hemodynamically stable, attention can be focused on the ureter-to-bladder anastomosis. Prior to skin incision a three-way catheter is inserted into the bladder. At this point in time, the Foley catheter tubing to the urine collection bag is clamped and the bladder is distended with antibiotic irrigation until distended adequately. Keep in mind that patients will have different volume of complete bladder distention depending on the amount of urine that they make. Over-distention can result in an extra- or intraperitoneal bladder rupture. The peritoneum is then reflected away from the bladder, and the serosal and detrusor are then divided for a length of 3 cm. The bladder is then entered with an #11 blade or Potts scissors and for 2 cm. The irrigation is aspirated and the Foley catheter clamp removed (Fig. 21.2). The ureter is cut to the appropriate length and the spatulated to match the bladder incision length. The ureter is then anastomosed to the bladder mucosa with 6-0 absorbable suture (Fig. 21.3). A 6 Fr × 12 cm double J closed-tip stent may be placed in the ureter to the pelvis and bladder prior to completion of the anastomosis. The detrusor is gently re-approximated over the anastomosis with interrupted 4-0 absorbable monofilament, with great care taken to avoid compressing the anastomosis.
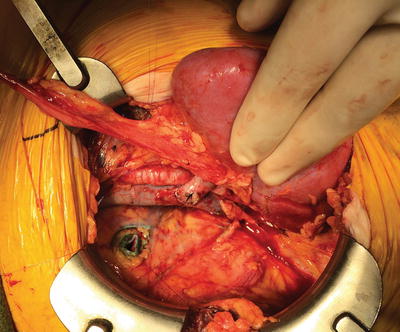
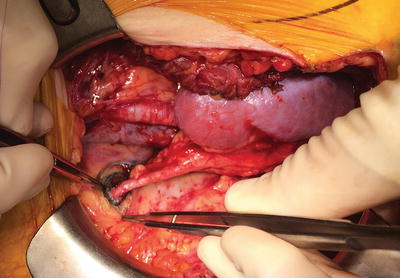
Fig. 21.2
Reperfused renal allograft with visualization of the venous anastomosis. The bladder has been opened in preparation for ureteral implantation
Fig. 21.3
Reperfused renal allograft with completed ureteral anastomosis
At this time thorough inspection of the operative field is undertaken to ensure hemostasis and appropriate positioning of the renal graft to avoid tension, torsion, or pressure on the renal artery or vein. A drain may be left if desired. The external oblique and anterior rectus sheath fascia is then closed in a running fashion. Subcutaneous layer is closed with absorbable suture and the skin with clips.
Related posts:
 Preoperative Evaluation and Preparation for Lung Transplantation
Anesthesia and Intraoperative Management of Renal Transplantation
Preoperative Evaluation and Preparation for Lung Transplantation
Anesthesia and Intraoperative Management of Renal Transplantation
 Intensive Care of the Deceased Multiorgan Donor: One Donor, Nine Lives
Intensive Care of the Deceased Multiorgan Donor: One Donor, Nine Lives
 Preoperative Liver Recipient Evaluation and Preparation
Preoperative Liver Recipient Evaluation and Preparation
 Technical Innovation and Visceral Transplantation
Postoperative Care of Heart Transplant Patients
Technical Innovation and Visceral Transplantation
Postoperative Care of Heart Transplant Patients

Full access? Get Clinical Tree


