(1)
Chennai Breast Centre, Chennai, India
Analysis of Mass Lesions
Mass lesions are space-occupying lesions in the breast seen in two views. Most breast cancers appear as masses, calcifications, or distortions or a combination of the three. Masses account for nearly half of all breast cancers detected on mammography. But not all mammographic masses are malignant.
History and physical examination findings are helpful. Proliferative lesions like fibroadenoma’s are likely to occur in younger women. Cysts are likely to occur more in the perimenopausal age group and they are more likely to be multiple. Sudden onset of a painful lump in the breast is probably due to a tension cyst. A rapidly enlarging mass in the third or fourth decades of life is more likely to be a phyllodes tumor. A long-standing, slowly enlarging lesion with a punctum on examination is likely to be a sebaceous cyst. If the patient has had history of surgery, trauma, or inflammation corresponding to the site of distortion or spiculations, then the possibilities of postsurgical or inflammatory scarring and traumatic fat necrosis exist.
Workup of Mass Lesions
Analysis of mammographic mass lesions involves assessment of shape, margins, and density. Apart from the standard CC and MLO views, spot compression with magnification will help in the assessment of masses (Fig. 6.1). Breast ultrasound is extremely useful in differentiating solid from cystic masses and in characterizing solid masses.
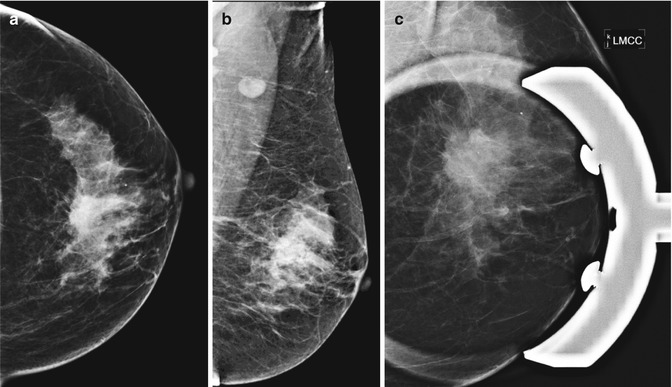
Fig. 6.1
(a, b) Left mammogram CC and MLO views showing a dense opacity with obscured margins in the upper quadrant. (c) Spot compression view delineates mass margins. The mass shows partly irregular and partly indistinct margins with associated microcalcifications—case of invasive ductal carcinoma
The ACR BI-RADS uses the following descriptors to describe a mass:
Shape | Margins | Density |
|---|---|---|
Round | Circumscribed | High |
Oval | Microlobulated | Equal |
Irregular | Obscured | Low |
Spiculated | Fat containing | |
Indistinct |
Shape
Majority of rounded or ovoid lesions are benign, like cysts, fibroadenoma, papilloma, benign phyllodes, Intramammary nodes, sebaceous cysts, etc. Malignant lesions are irregular because they are infiltrative in nature. Less than 5 % of round or ovoid lesions are malignant. Well-circumscribed rounded malignant lesions are usually invasive carcinomas with special features such as mucinous or medullary carcinoma. Intracystic cancers, triple negative malignancies, malignant phyllodes, metaplastic carcinomas, lymphomas, and metastasis to breast also present as rounded lesions (Fig. 6.2a–c).
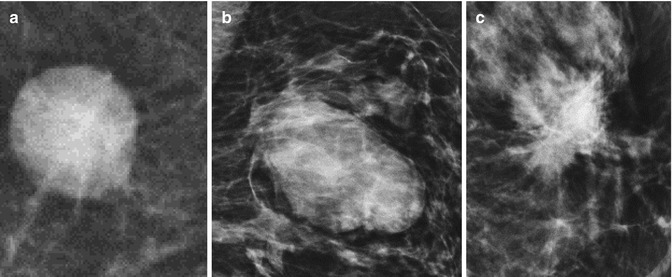
Fig. 6.2
(a–c) Mammographic images. (a) Round lesion. (b) Oval that includes 2 or 3 gentle lobulations. (c) Irregular-shaped lesion
Apart from the shape, the margins and the density of the mass are helpful in differentiating benign from malignant tumors. Spot compression and magnification views are useful in defining shape and margins.
Margins
A sharp margin with a capsule is usually seen in lipoma and oil-containing cysts. These are certainly benign. Halo sign is a fine 1-mm radiolucent line that surrounds circumscribed masses. It may be complete or partial and, when present, suggests the possibility of a benign lesion (Fig. 6.3a, b). Not all masses with halo sign are benign. Gordenne and Machair described a broad band of lucency measuring 5–20 mm that surrounds a malignancy due to mach band effect.
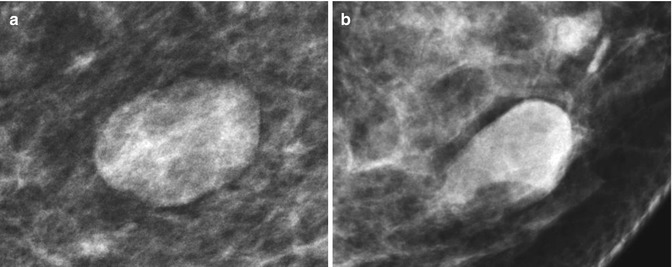
Fig. 6.3
(a, b) Mammogram images showing well-circumscribed ovoid opacities with (a) complete and (b) partial halo sign
Sharply outlined margins with no capsule or halo sign may be seen in some masses like cysts, intracystic cancers, and phyllodes.
Sometimes, overlapping fibroglandular tissues may obscure a margin, making it difficult to analyze the margin. Spot compression and magnification views can help in the contour analysis.
Indistinct margins are worrisome and are strongly suspicious for malignancy. It may represent tumor invading the surrounding structures, and therefore, masses with indistinct margins require further evaluation with additional spot compression and magnification views and ultrasound examination. Sometimes benign lesions like papillomas, abscesses, complex cysts, and some fibroadenomas also have indistinct margins. Ancillary tools such as breast ultrasound are required in the workup of these lesions.
Masses with microlobulated small undulations in the margin or spiculated margins are highly suspicious for malignancy. These lesions will certainly necessitate breast ultrasound for further characterization and histopathology (Fig. 6.4a–e).
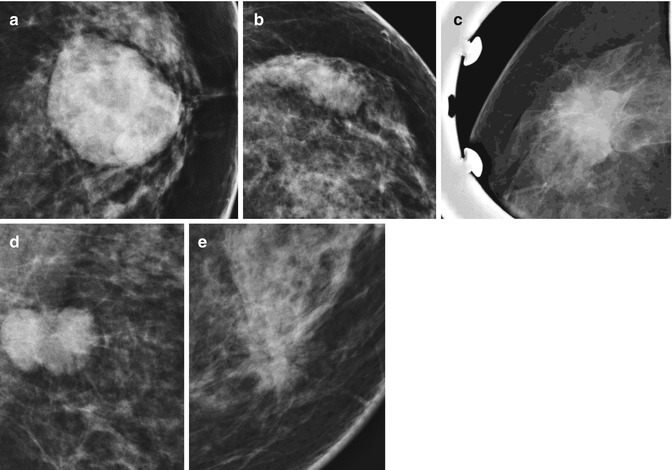
Fig. 6.4



(a–e) Mammographic images showing (a) a well-circumscribed margin, (b) obscured margin, (c) indistinct margins, (d) microlobulated margin, and (e) spiculated margin
Related posts:





Full access? Get Clinical Tree
