Key Clinical Questions
What are the presenting symptoms of a severe allergic reaction or anaphylaxis?
What are the most common causes of allergic reactions?
How do anaphylactic and anaphylactoid reactions differ? How are they treated?
What conditions mimic allergic reactions?
What are the most common types of allergic reactions among hospitalized patients?
Which patients require outpatient referral to an allergist?
Introduction
Allergic reactions result from an aberrant immune response to an inciting antigen or allergen. The subsequent inflammatory state produces a wide range of clinical symptoms. Anaphylaxis, the most extreme form of allergic reaction, refers to sudden, severe, and potentially fatal hypersensitivity developing in seconds to minutes after exposure.
Epidemiology
It is estimated that anaphylaxis accounts for 1 in 2000 ambulance trips and is fatal in as many as 0.7 to 2% of cases. Two epidemiologic studies demonstrated that 1 out of every 2700–5100 hospitalizations can be linked to anaphylactic reactions. While the term allergy denotes an immediate hypersensitivity reaction involving immunoglobulin E (IgE) antibody, a large number of severe allergic reactions are not IgE mediated. These “anaphylactoid” reactions are clinically indistinguishable from anaphylaxis and include hypersensitivity to radiocontrast dye, angiotensin-converting enzyme inhibitors, and opiates.
Clinical Presentation
Patients experiencing allergic reactions may vary widely in their clinical presentations. Factors affecting the clinical picture include the amount and persistence of antigen, its route of entry, and the end organ response to vasoactive mediators. The majority of allergic reactions manifest as skin findings, such as flushing, pruritus, and transient urticaria. In more severe reactions, a larger number of deep dermal mast cells are recruited, resulting in angioedema.
The onset of anaphylactic reactions can occur minutes to hours after exposure to an allergen and denotes the systemic activation of mast cells. Aside from the cutaneous manifestations, patients may experience respiratory manifestations (hoarseness of voice, dyspnea, wheezing, cough, and chest tightness), gastrointestinal manifestations (nausea, vomiting, colicky abdominal pain, and diarrhea), and cardiovascular manifestations (peripheral vasodilation, reflex tachycardia, and hypotension with resultant cardiovascular collapse).
|
Pathophysiology
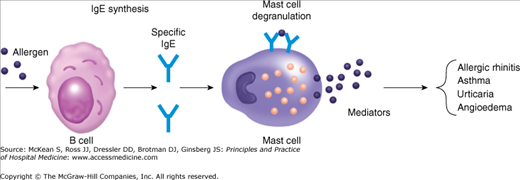
When the body is exposed to an antigen, a specific IgE antibody is formed that binds to high-affinity receptors, called Fc epsilon type I, located on mast cells and basophils. Upon reexposure to that allergen cross-linking of cell-bound IgE antibody occurs, resulting in Fc epsilon receptor aggregation and activation. The resultant mast cell degranulation leads to release of inflammatory mediators such as histamine, prostaglandins, tryptase, platelet activation factor, and leukotrienes, all directly contributing to the allergic response through smooth muscle contraction, bronchoconstriction, vasodilation, increased vascular permeability, and edema (Figure 237-1). Allergic reactions mediated by T-helper type 2 (TH2) cells (a subset of CD4+ T-cells) preferentially produce interleukins (IL) 4, 5, and 13; all powerful mediators of allergic response. IL-4 promotes B-cell activation and T-cell proliferation and is also responsible for CD4+ T-cell differentiation to TH2 cells. IL-5 recruits and activates eosinophils, contributing to the late phase of allergic inflammation. The functions of IL-13 overlap considerably with those of IL-4 and it synergizes with IL-4 in the production of IgE antibody by B cells.
Differential Diagnosis
Several disease processes can mimic the clinical features of anaphylaxis. Vasovagal reactions, cardiac arrhythmias, bronchoconstriction, and hypoglycemia, for example, can all be associated with hypotension, pallor, diaphoresis, dyspnea, and wheezing. Pruritis and urticaria may serve as distinguishing factors as they are absent in these mimicking conditions. Viral exanthems and enanthems, depending on their timing, can also be mistaken for hypersensitivity reactions, but they do not manifest itching.
|
In addition to catalyzing the conversion of angiotensin I to angiotensin II, angiotensin-converting enzyme (ACE) breaks down bradykinin, in both tissues and plasma, into inactive peptide fragments. Patients taking ACE-inhibitors, therefore, have elevated levels of bradykinin, which stimulates cough receptors and can lead to bouts of angioedema. Most reactions occur in the first week following initiation of the drug, but up to 40% can occur months or even years after starting the drug. Typically patients present with angioedema involving the lips, tongue, uvula, soft palate, and, much less commonly, bowel, manifesting as acute abdominal pain.
Antihistamines are ineffective, and systemic corticosteroids offer limited benefit in the treatment of ACE-inhibitor-induced angioedema. Symptoms improve with discontinuation of the drug, and patients should not be rechallenged with a different ACE-inhibitor or treated at a lower dose. Most patients with ACE-inhibitor angioedema can tolerate an angiotension receptor blocker (ARB). However, treatment needs to be individualized given rare case reports of angioedema with these agents. If there is a strong indication for the ARB (eg, diabetic nephropathy, heart failure) and the episode of angioedema was non–life threatening, then an ARB can be prescribed with caution.
|
Hereditary angioedema (HAE), a rare autosomal dominant disease characterized by a low or nonfunctioning C1 esterase inhibitor can present with episodes of angioedema involving the face, larynx, lips, abdomen, genitalia, and extremities. While attacks may occur in childhood, typically the disease manifests in the second or third decade of life. Aside from prior bouts of angioedema, patients will often endorse a family history of similar attacks. If there is diagnostic uncertainty, a C4 level is a cost-effective screening test. A normal C4 level effectively rules out HAE since a low or nonfunctional C1 esterase inhibitor results in the activation of C4. The C2 level correlates with activity of disease.
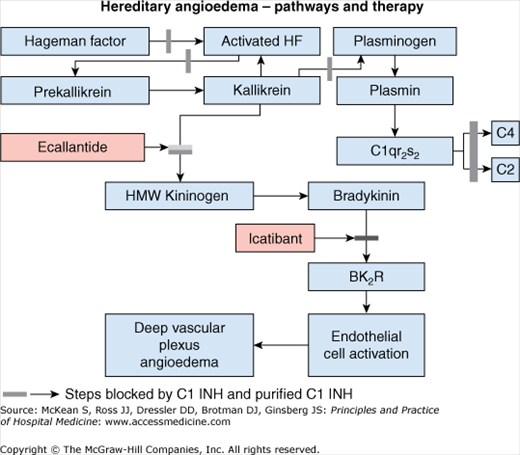
While HAE is a rare disorder clinicians must distinguish it from anaphylaxis. During episodes of HAE the cascade produces vasoactive kinin proteins such as kallikrein and bradykinin (Figure 237-2); mast cells are not activated; hence patients do not manifest pruritus or concomitant urticaria. Therefore, traditional therapies with antihistamines, steroids, and epinephrine have little therapeutic utility. Acute episodes are managed with supportive care and the administration of pasteurized C1 esterase inhibitor concentrate. C1 esterase inhibitor is derived from human plasma and bears infection transmission risks similar to other blood product transfusions. A new formulation—pasteurized, nanofiltered C1 esterase inhibitor concentrate—awaits U.S. Food and Drug Administration (FDA) approval for acute attacks but is currently recommended for prophylactic use. Ecallantide, a potent inhibitor of plasma kallikrein, has FDA approval for treatment of acute attacks. Subcutaneous administration of icatibant, a peptide inhibitor of the bradykinin B2 receptor, is approved in Europe for treatment of acute attacks but is not yet FDA approved.
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist

Full access? Get Clinical Tree


