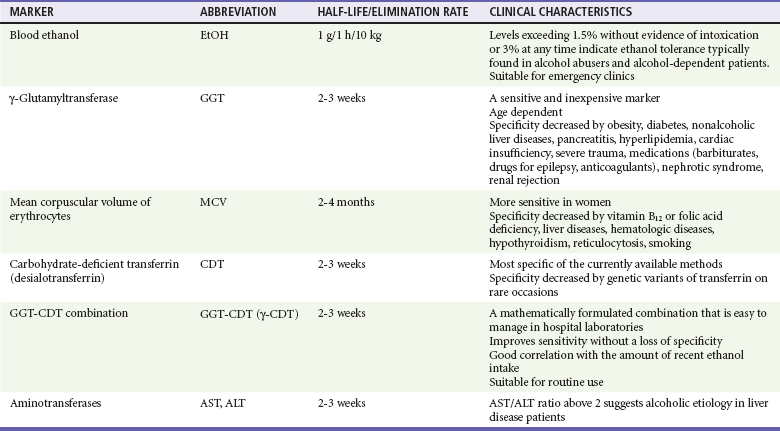
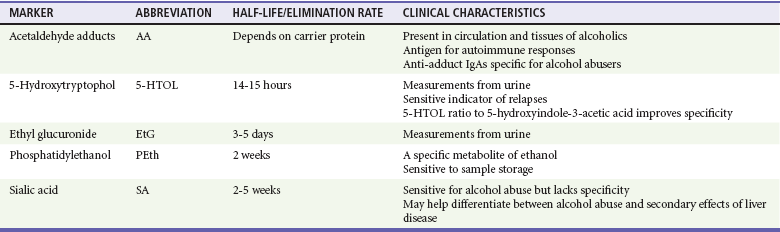
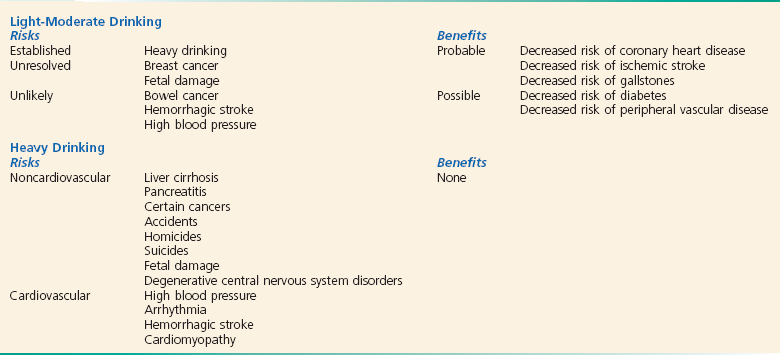
Chapter 185 The disastrous effects and widespread incidence of alcoholism are well known to the emergency physician. Almost all societies that consume alcohol show related health and social problems.1 Motor vehicle collisions, drowning, suicides, homicides, divorce, violent crime, child abuse, unemployment, and disruption of the family are often either directly or indirectly associated with excessive alcohol consumption. The tragic effects of alcohol not only affect the individual drinker but also have far-reaching implications for the family, community, and workplace. In the United States, an estimated 7.6 million visits to the emergency department (ED) a year are related to alcohol, accounting for 7.9% of all ED visits.2 Table 185-1 lists the causes of death related to alcohol abuse. Table 185-1 Causes of Death Related to Alcohol Abuse Modified from Miranda-Mendez A, Lugo-Baruqui A, Armendariz-Borunda J: Molecular basis and current treatment for alcoholic liver disease. Int J Environ Res Public Health 7:1872-1888, 2010. Alcohol is the most common recreational drug taken by Americans, and per capita consumption is increasing. An estimated 18 million alcoholics live in the United States; with more than 85,000 alcohol-related deaths each year, resulting in 2.3 million years of potential life lost,3 alcohol is the third leading cause of preventable death in the United States.4 Alcoholism permeates all levels of society and is a preventable cause of morbidity and mortality, with a cost to the nation estimated to be greater than $185 billion annually.5 Alcohol dependence is associated with major physiologic consequences and life impairment. Dependence can be identified as repetitive problems, affecting three or more areas of life, and about 80% of people who are diagnosed with dependence at any point still have alcohol-related problems when they are assessed a year or more later.6 Dependence criteria are reliable across different ages, sexes, and most cultural groups. Alcohol abuse is defined by the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), as one or more problems with functioning in a 12-month period in a person without dependence: failure in obligations; alcohol use in hazardous situations; recurrent legal problems; or continued use despite social or interpersonal problems.7 The AUDIT-C Screening Questionnaire: 1. How often do you have a drink containing alcohol? Never (0 points), monthly or less (1 point), two to four times a month (2 points), two or three times a week (3 points), four or more times a week (4 points) 2. How many drinks containing alcohol do you have on a typical day when you are drinking? 3. How often do you have six or more drinks on one occasion? Never (0 points), less than monthly (1 point), monthly (2 points), weekly (3 points), daily or almost daily (4 points) Scoring: The sum of scores for the three questions results in an AUDIT-C score of 0 to 12 points. Blood tests can be useful if the history is in doubt and can also help patients recognize that alcohol has adversely affected their health. One such marker is γ-glutamyltransferase, an enzyme important in amino acid transport. Results of at least 35 units/L indicate the probability of heavy drinking. A second test is for carbohydrate-deficient transferrin, which measures a change in the structure of a proportion of transferrin that is likely to occur with heavy drinking during a long period; a result of 20 units/L or more indicates heavy drinking. Tests of liver function that measure aspartate transaminase (AST) and alanine transaminase (ALT) can identify heavy drinking and alcohol-use disorders with sensitivities of 25 to 45% and specificities as high as 90%. A ratio of AST to ALT higher than 2, especially if concentrations of these enzymes do not exceed 400 units/L, suggests alcoholic hepatitis. Although many newer biomarkers are not yet available, these newer markers (acetaldehyde adducts) rely on protein modifications by acetaldehyde and play an important role in the pathogenesis of tissue damage in alcoholics (Tables 185-2 and 185-3). Table 185-2 Current Biomarkers in Alcoholism From Niemelä O: Biomarkers in alcoholism. Clin Chim Acta 377:39-49, 2007. Table 185-3 Emerging Biomarkers in Alcoholism From Niemelä O: Biomarkers in alcoholism. Clin Chim Acta 377:39-49, 2007. A precise definition of alcoholism is difficult. A proposed definition encompassing the features of alcoholism is “a primary chronic disease with genetic, psychosocial, and environmental factors influencing its development and manifestations.” The disease is often progressive and fatal. It is characterized by impaired control over drinking, preoccupation with and use of alcohol despite adverse consequences, and distortions in thinking, most notably denial. Each of these symptoms may be periodic or continuous.8 Alcoholism is present when drinking adversely affects an individual’s physical health, ability to function in society, or interpersonal relationships. Men: more than 14 drinks per week or more than 4 drinks per occasion Women: more than 7 drinks per week or more than 3 drinks per occasion Age older than 65 years: more than 7 drinks per week or more than 1 drink per occasion Harmful drinkers present with negative consequences related to alcohol. The natural history of alcoholism is variable, and it may appear in any patient despite age or social status. The age at onset of alcoholism continues to decrease. Up to 6% of high school seniors drink daily, and it is not unusual to see children younger than 16 years who have already graduated from an alcohol detoxification program.9 Many individuals also begin drinking heavily after the age of 60 years. The DSM-IV has two categories for substance disorders that include alcohol abuse: (1) substance abuse and (2) substance dependence.7 The chronic substance abuse of alcohol eventually leads to acquired tolerance, a condition in which larger and larger doses of alcohol are required for the same effect. The absorption and elimination rates of alcohol vary by individual and depend on many factors: diet, gender, body weight and habitus, speed of consumption, gastric motility, presence of food in the stomach, smoking history, age, whether the person is a chronic alcohol consumer with enzyme induction and high-activity MEOS, advanced cirrhosis, presence of ascites, and state of nourishment.10 There is enormous variation among patients in the rate of disappearance of ethanol from the blood, ranging from 9 to 36 mg/dL per hour in published data. Although the clearance rate may be as high as 36 mg/dL per hour in some chronic drinkers, 20 mg/dL per hour is a reasonable rate to assume in a typical intoxicated ED patient. This holds true for adults, adolescents, and children.11 Physiologic effects vary directly with the blood alcohol level (Table 185-4). Diminished fine motor control and impaired judgment appear with alcohol concentrations as low as 20 mg/dL (0.02 mg%), but wide individual variability exists. Chronic alcoholics can exhibit impressive tolerance. The blood alcohol concentration of a person cannot be accurately determined without quantitative testing. More than 50% of the adult population is obviously intoxicated with a level of 150 mg/dL (0.15 mg%). As the ethanol level rises, the patient’s level of consciousness declines, eventually ending in coma. Death is caused by aspiration or respiratory depression. Table 185-4 Physiologic Effects and Blood Alcohol Levels *These effects are for the occasional drinker. Chronic drinkers can function at much higher alcohol concentrations because of tolerance. On the other hand, patients may become comatose with low levels of alcohol in mixed alcohol-drug overdose. Alcohol through passive diffusion will be present anywhere there is water in the body. Hence, expired breath alcohol or saliva can be used to obtain a reliable approximation of blood alcohol concentration in a cooperative patient. This value can be used as a rapid screen for alcohol intoxication.12,13 Glucose (dextrose, 25 g IV) produces a dramatic response in alcohol-induced hypoglycemic patients. Unlike hypoglycemia of other causes, alcohol-induced hypoglycemia may be unresponsive to glucagon because of depleted liver glycogen stores. Although Wernicke’s encephalopathy is a medical emergency, alcohol-induced hypoglycemia is a much more common condition with serious and permanent morbidity if it is left untreated. Therefore, thiamine can be given in a timely fashion, but glucose therapy should not be delayed.14 The neurophysiology of alcohol withdrawal is complex and not fully understood. Chronic alcohol consumption has a depressant effect on the central nervous system (CNS). The hallmark of alcohol withdrawal is CNS excitation with increased cerebrospinal fluid, plasma, and urinary catecholamine levels. Chronic alcohol consumption affects central adrenergic alpha receptors, glutamate, central adrenergic beta receptors, the inhibitory neurotransmitter γ-aminobutyric acid (GABA), and dopamine turnover.15 Isbell’s classic study in 1955 confirmed the relationship between alcohol and the withdrawal syndrome.16 He documented that the severity of signs and symptoms depends on both the dose and the duration of ethanol consumption. The withdrawal syndrome may occur any time after the blood alcohol level starts to fall. Therefore, only a reduction, not the abrupt cessation, of ethanol intake may result in withdrawal. Minor alcohol withdrawal occurs as early as 6 hours and usually peaks at 24 to 36 hours after cessation of or significant decrease in alcohol intake. It is characterized by mild autonomic hyperactivity: nausea, anorexia, coarse tremor, tachycardia, hypertension, hyper-reflexia, sleep disturbances (e.g., insomnia, vivid dreams), and anxiety.17 Major alcohol withdrawal occurs after more than 24 hours and usually peaks at 50 hours but occasionally takes up to 5 days to be manifested after the decline or termination of drinking. The syndrome is characterized by pronounced anxiety, insomnia, irritability, tremor, anorexia, tachycardia, hyper-reflexia, hypertension, fever, decreased seizure threshold, auditory and more commonly visual hallucinations, and finally delirium.18 Benzodiazepines.: The benzodiazepines have superior anticonvulsant activity, have the least respiratory and cardiac depressive effect of all the CNS depressants, and can be given parenterally in the uncooperative patient. By interacting with receptors linked to the GABA-associated chloride ion channel, benzodiazepines substitute for the withdrawal of the GABA-potentiating effect of alcohol and abate withdrawal signs and symptoms.19 Numerous benzodiazepines have been studied, but there is no evidence of clear superiority of any one benzodiazepine. As one dosing regimen, diazepam, 5 mg IV every 5 to 10 minutes (2.5 mg/min), can be given in major withdrawal until the patient is calm. The dose can be repeated in 5 to 10 minutes. If the second dose of 5 mg is not working, consider 10 mg for the third and fourth doses every 5 to 10 minutes. If this is not effective, consider 20 mg for the fifth and subsequent dose until adequate sedation is obtained.20,21 Butyrophenones.: Haloperidol, a dopamine antagonist, can be considered in patients with major alcohol withdrawal or delirium tremens not responding to intravenous benzodiazepines. Haloperidol has little effect on myocardial function or respiratory drive, and its safety and efficacy by the intravenous, intramuscular, or oral route in the ED have been established. Haloperidol has no anticonvulsant properties; however, extrapyramidal effects may be seen. Caution should be used in patients who may be susceptible to a prolonged QTc. Droperidol has effects similar to those of haloperidol. Despite the 2001 Food and Drug Administration black box warning for QTc prolongation and torsades de pointes after droperidol use, droperidol remains a safe and effective treatment for agitated patients.22 Among the many medical problems related to alcohol abuse, the differential diagnosis and management of seizures remain among the most challenging and controversial (Box 185-1). Patients presenting to the ED with seizures should be questioned about alcohol intake. Of seizure patients presenting to an ED, 20 to 40% will have their seizures related to alcohol use or abuse.23 Alcohol is a causative factor in 11 to 24% of patients with status epilepticus.24,25 In states where alcohol sales are restricted on Sundays, EDs see a spike in alcohol-related seizures on Mondays.26 The primary consideration in the initial care of seizure patients who use alcohol is the recognition of treatable, life-threatening causes. These causes include but are not limited to CNS infection, metabolic disorders, and intracranial hemorrhage. Alcohol may act in one of several ways to produce seizures in patients with or without underlying foci: by its partial or absolute withdrawal after a period of chronic intake, by an acute alcohol-related metabolic disorder (e.g., hypoglycemia, hyponatremia), by creation of a situation leading to cerebral trauma, by precipitation of seizures in patients with idiopathic or post-traumatic epilepsy, or by lowering of the seizure threshold in patients with prior existing intracerebral disease states. Moreover, alcoholics are more susceptible to other disorders associated with seizures, including neurosyphilis, acquired immunodeficiency syndrome (AIDS), brain abscess, and meningitis.27–29 Descriptions of alcohol withdrawal seizures are based on data collected by Victor and Brausch.30 Seizures occurred 6 to 48 hours after the cessation of drinking. Ninety percent had one to six generalized tonic-clonic seizures. Sixty percent experienced multiple seizures within a 6-hour period. However, seizure recurrence can be reduced to 3% with lorazepam administration after the initial seizure.31 The incidence of partial seizures, common with post-traumatic epilepsy, is increased in alcohol withdrawal. The term alcohol withdrawal seizure is reserved for seizures with the characteristics described by Victor and Brausch.30 The term alcohol-related seizure is used to refer to all seizures in the aggregate associated with alcohol use, including this subset of alcohol withdrawal seizure. New-Onset Alcohol-Related Seizures Patients with new-onset alcohol-related seizure should be thoroughly evaluated. This includes alcoholics who claim to have had seizures but for whom no documentation or an appropriate work-up is available. Metabolic disorders, toxic ingestion, infection, and structural abnormalities should be considered. Laboratory and radiographic testing to include electrolyte values and blood urea nitrogen, creatinine, glucose, and anticonvulsant levels and brain computed tomography (CT) scan may be necessary. Of 259 patients presenting with their first alcohol-related seizure, clinical management was changed in 3.9% on the basis of head CT results.32 The risk of seizure increases significantly in alcoholic patients with manifestations of alcohol withdrawal who relate a history of alcohol withdrawal seizure.33,34 Detoxification with benzodiazepines reduces alcohol withdrawal seizure and should be initiated early because most seizures occur within the first 24 hours after alcohol withdrawal. An initial dose of 2 mg of lorazepam or 5 mg of diazepam can be given intravenously. These doses frequently need to be repeated.35 The patient should be observed for 4 to 6 hours before discharge is considered. The prescription of benzodiazepines or antiepileptic drugs on discharge carries its own hazards. Benzodiazepines (other than a short 3- to 6-day tapering dose for withdrawal) may increase the potential risk of addiction. In a noncompliant patient, antiepileptic drugs, such as phenytoin, may paradoxically increase the number of seizures. The poorly compliant alcoholic patient may do better without outpatient anticonvulsants for a concurrent seizure disorder.33 The ideal disposition is referral to a detoxification or rehabilitation unit. Partial seizures account for 24 to 51% of alcohol-related seizures.36 Conversely, studies have shown that 17 to 21% of patients with partial alcohol-related seizure have structural lesions: hematomas, tumors, vascular abnormalities, or stroke.37 These primary causes of partial alcohol-related seizure, such as prior head trauma, may be easily missed in the history taking. As a result, an emergent CT scan is indicated to evaluate new-onset partial seizures. The patient with a history of a focal alcohol-related seizure who has been previously evaluated does not require an emergency CT scan, provided a return to baseline occurs promptly. A patient presenting with a focal alcohol-related seizure with subsequent normal neuroimaging findings can be managed with supportive care, observation for 4 to 6 hours, and a benzodiazepine for withdrawal signs or symptoms. Appropriate follow-up should be arranged. Phenytoin has no significant benefit over placebo in prevention of recurrence of uncomplicated (e.g., no old subdural) alcohol withdrawal seizure. Considering the risks of phenytoin and no demonstrated benefit in the setting of alcohol withdrawal seizure, it is not indicated for the treatment of alcohol withdrawal seizure. The sudden withdrawal of phenytoin may potentiate the convulsive effects of alcohol withdrawal.23,38 A patient currently taking antiepileptic drugs for an antecedent seizure disorder who presents with a seizure while intoxicated falls into a different category. Such an episode could be an isolated event in a usually compliant patient without a history of chronic alcohol abuse. In this patient, a seizure in the setting of a subtherapeutic antiepileptic drug level may represent the consequences of noncompliance with antiepileptic medication or sleep deprivation versus alcohol withdrawal seizure.33 Acute and chronic ethanol consumption can affect the mechanical function of the heart, produce dysrhythmias, and exacerbate coronary artery disease (CAD). It may alter myocardial function by direct toxic effects, by associated hypertension, or indirectly by altering specific electrolytes. Acute intoxication can decrease cardiac output in both alcoholic and nonalcoholic patients with preexisting cardiac disease.38 Studies have linked moderate alcohol consumption (two to four drinks per day in men and one or two in women) to a protective effect from CAD. Low to moderate alcohol consumption decreases platelet aggregation, raises plasma levels of endogenous tissue plasminogen activator,39 and lowers insulin resistance. Experimental data suggest that alcohol may have antioxidant properties, produce effects on smooth muscles through interactions with nitric oxide, and alter plasma total homocysteine levels.40,41 The red versus white wine hypothesis rests on human studies showing short-term cardiovascular benefits achieved by de-alcoholized red but not white wine and many studies on isolated tissues or organs assessing the effects of polyphenols in red wine, especially resveratrol. Therefore, red wine potentially has beneficial effects beyond alcohol content.42 Studies suggest that moderate alcohol consumption, through a reduced risk of CAD, may also protect individuals from congestive heart failure (Box 185-2).43 All of these beneficial effects are lost in heavy drinkers, in whom chronic alcoholism is associated with hypertension and congestive cardiomyopathy. Up to one third of chronic alcoholic patients have left ventricular dysfunction demonstrated by radionuclide ventriculography, usually coexisting with skeletal muscle disease. Those who stop using alcohol may have an improved ejection fraction during the course of 3 years.44 Although the primary functional abnormality of alcoholic cardiomyopathy was thought to be a depression in systolic function, it is now appreciated that an impairment in diastolic function is present in one third of alcoholics who have a normal systolic function; in many, systolic dysfunction and diastolic dysfunction coexist. Excess alcohol consumption affects not only the cardiomyocytes but striated skeletal muscle as well. Women appear to be more sensitive than men to the toxic effects of alcohol on striated muscle and are at greater risk for cardiomyopathy and myopathy as well as for skeletal myopathy for any given lifetime amount of alcohol.44 Heavy alcohol consumption has a detrimental effect on those with preexisting CAD. It can reduce exercise tolerance, induce coronary vasoconstriction, and raise heart rate and blood pressure.45 Additive cardiovascular effects of ethanol and nicotine contribute to dysrhythmias and sudden death in patients with CAD. In one study, nearly half the patients with alcohol withdrawal had prolongation of the QT interval. Prolonged QT can precipitate a dysrhythmia, resulting in sudden death.46 There is an increased incidence of sudden death among heavy drinkers regardless of concomitant CAD or smoking. Alcohol also affects cardiac function indirectly by lowering potassium and magnesium levels. Data from the Framingham Heart Study indicate that patients with lower levels of potassium and magnesium have higher rates of dysrhythmias.47 Alcohol reduces the mobilization of alveolar macrophages and their bactericidal capacity. Their impairment is greatest in alcoholics with hepatic cirrhosis. In alcoholic patients, the lungs are more vulnerable to oxidative stress and injury. There is evidence that chronic alcohol consumption decreases the level of glutathione, promoting inflammation and remodeling of the lung tissue.48 These effects, along with aspiration, decreased airway sensitivity, concomitant smoking, and malnutrition, probably account for the increased incidence of pneumonia, particularly lobar pneumonia, among alcoholic patients.49 Alcohol abuse is also associated with an increased likelihood of intensive care unit admission and a longer hospital length of stay than for non-alcoholic patients with community-acquired pneumonia.50 At least 80% of alcoholics are smokers, making it difficult to distinguish between alcohol-induced and tobacco-induced injury to the lungs. The high prevalence of respiratory disease in alcoholics is largely caused by smoking. Patients with sepsis and chronic alcohol abuse are at least twice as likely to require mechanical ventilation and have a twofold to fourfold risk for development of the acute respiratory distress syndrome.50 Alcohol induces bronchospasm in some asthmatics and increases ventricular ectopy and sleep apnea in patients with chronic obstructive pulmonary disease. Alcoholic patients with hepatic cirrhosis can have hypoxemia as a result of precapillary shunting in their lungs. Hyperventilation and respiratory alkalosis are also seen with hepatic cirrhosis. One or two drinks per day has been found to decrease the risk of pulmonary embolus and deep venous thrombosis in elderly patients.51
Alcohol-Related Disease
Perspective
Epidemiology
1
Mouth and oropharynx cancer
2
Alcohol use disorders
3
Ischemic heart disease
4
Liver cirrhosis
5
Road traffic accidents
6
Poisonings
7
Falls
8
Intentional injuries
Diagnosis
Alcohol Screening Questionnaires
Definition and Natural History
Principles of Disease: Metabolism of Alcohol
BLOOD ALCOHOL CONCENTRATION (mg/dL)
EFFECTS*
20-50
Diminished fine motor control
50-100
Impaired judgment; impaired coordination
100-150
Difficulty with gait and balance
150-250
Lethargy; difficulty sitting upright without assistance
300
Coma in the novice drinker
400
Respiratory depression
Management
Alcohol Withdrawal Syndrome
Clinical Features
Management
Alcohol-Related Seizures
Alcohol Withdrawal Seizures
Patients Presenting with Normal Findings on Neurologic Examination
Seizures in the Alert Patient with a History of Seizures during Prior Withdrawal
Patients with an Abnormal Neurologic Presentation
Patients Taking Phenytoin-Anticonvulsant
Other Clinical Features and Management
Pulmonary Effects





Full access? Get Clinical Tree


