Airway Management and Endotracheal Intubation
Elifce O. Cosar
Adam D. Currier
I. GENERAL PRINCIPLES
A. Maintenance of adequate ventilation and pulmonary gas exchange is very important in critically ill patients. Airway management in intensive care patients differs significantly from routine surgical procedures in the operating room.
B. Critical care physicians should be familiar with the equipment and the techniques to maintain and secure the airway.
II. ANATOMY. The airway is divided into the upper airway and lower airway.
A. Nose.
The nose serves a number of functions: respiration, olfaction, humidification, filtration, and phonation.
B. Pharynx.
The pharynx extends from the base of the skull to the level of the cricoid cartilage.
C. Larynx.
1. The larynx lies in the adult neck opposite the third through sixth cervical vertebrae.
2. The laryngeal skeleton consists of hyoid bone and nine cartilages. These are the unpaired thyroid, cricoid, and epiglottis and the paired arytenoid, corniculate, and cuneiform cartilages. The cricoid cartilage is the only structure that completely encircles the airway.
3. Two nerves that are branches of the vagus innervate the larynx.
a. The external branch of superior laryngeal nerve supplies motor innervation to the cricothyroid muscle. All other motor supply to the laryngeal muscles is provided by the recurrent laryngeal nerve.
b. The internal branch of the superior laryngeal nerve provides sensation above the cords. Sensory innervation below the cords is supplied by the recurrent laryngeal nerve.
D. Trachea.
1. The adult trachea begins at the cricoid cartilage. It is 10 to 20 cm long.
2. It divides into right and left main bronchi at the level of fourth and fifth thoracic vertebrae. The right main bronchus is wider and shorter and takes off at a less acute angle than the left, thus making right main bronchus intubation more likely.
III. EVALUATION OF THE AIRWAY
A. Several clinical criteria can be assessed.
1. Mouth opening.
2. Mallampati classification (Fig. 1-1).
3. Head and neck movement.
4. Ability to prognath (i.e., to bring the lower incisors in front of the upper incisors).
5. Thyromental distance.
6. Body weight.
7. Neck circumference.
8. Previous history of difficult intubation (single most reliable predictor of a difficult airway).
B. Difficult airway in some patients will remain undetected despite the most careful airway examination.
C. Cervical collars, halo devices, trauma to the mandible or neck, morbid obesity, pregnancy, acromegaly, burns, and obstructive sleep apnea may signal a difficult airway.
D. Age >55, body mass index >26, snoring, presence of a beard, lack of teeth, Mallampati class III or IV, abnormal mandibular protrusion test, and male gender are independent clinical risk factors for difficult mask ventilation.
IV. AIRWAY EQUIPMENT
A. An oxygen source, face masks of different sizes, a bag-valve ventilation device, suction catheters, and suction source with canister and tubing.
B. Oral and nasopharyngeal airways (Fig. 1-2).
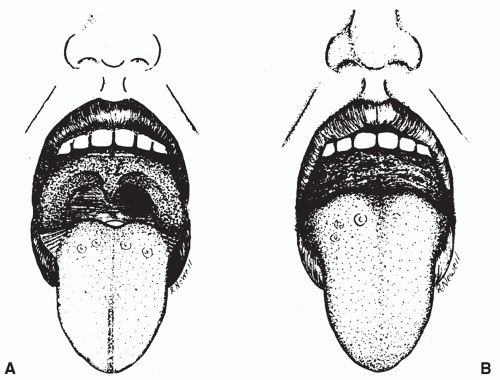 Figure 1-1. Mallampati classification: class I airway, faucial pillars, soft palate, and uvula can be visualized (A); class II airway, faucial pillars, and soft palate can be visualized but the uvula is masked by the base of the tongue; and class III airway, only the soft palate can be visualized. The patient (B) has a class III airway, which is one of the predictors of difficult orotracheal intubation. (From Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J 1985;32:420, with permission.) |
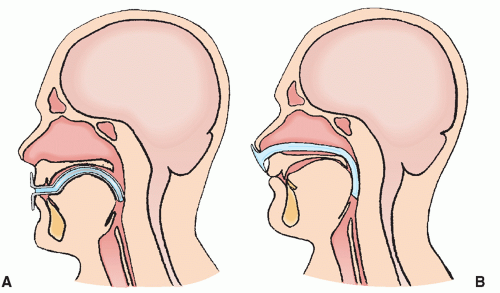 Figure 1-2. A: The proper position of the oropharyngeal airway. B: The proper position of the nasopharyngeal airway. (Reprinted Dorsch JA, Dorsch SE. A practical approach to anesthesia equipment. Philadelphia: Lippincott Williams & Wilkins, 2011:254-259, with permission.) |
Related posts:





Full access? Get Clinical Tree


