 Patient Positioning
Patient Positioning
 Direct Laryngoscopy
Direct Laryngoscopy
I. INTRODUCTION: Endotracheal intubation is indicated in the setting of acute respiratory failure (hypoxemic or hypercarbic) when noninvasive positive pressure ventilation (NIPPV) has failed or is contraindicated, obtundation (Glasgow Coma Score <8), airway obstruction, or anticipation of compromised airway patency due to trauma, edema, or other etiologies. This chapter will review airway evaluation, advanced airway placement/maintenance, and evaluation for withdrawal of advanced airway support.
II. INDICATIONS FOR ADVANCED AIRWAY: Intact respiratory function requires a central drive to breathe, appropriate respiratory neuromuscular function, a patent upper airway, the ability to protect the airway from aspiration, and effective ventilation and perfusion matching. Placement of an endotracheal tube (ETT) allows ventilation of a patient who lacks a respiratory drive, can support the work of breathing in a patient who is weak, provides an opening through an upper airway that may be prone to collapse, mitigates large volume aspiration, and, by using positive pressure, reexpands atelectatic lung regions that contribute to ventilation/perfusion mismatch.
III. ASSESSMENT OF NEED FOR AN ADVANCED AIRWAY
A. Cardiopulmonary Resuscitation: Per ACLS guidelines, bag mask ventilation with 100% inspired oxygen is required. If bag-mask ventilation is inadequate, an advanced airway (ETT, supraglottic airway [SGA]) should be placed without interruption of chest compressions.
B. Decreased Level of Consciousness: Intubation may be required due to airway obstruction, decreased respiratory drive, and risk of aspiration. Though GCS <8 is classically taught as an indication for intubation, significant risk of aspiration exists with GCS scores >8, and thus the presence of gastro-esophageal reflux disease (GERD), esophageal sphincter dysfunction, and full stomach may justify intubation in a stuporous patient.
C. Pulse Oximetry: Continuous monitoring aids the assessment of patients with hypoxia. While more quantifiable and reliable than the appearance of cyanosis, there is no number that absolutely warrants intubation. Oxygen saturations below 88% usually require evaluation and may require intervention.
D. Respiratory Patterns:
1. Respiratory rate (RR)/Tidal volume (TV):
a. ↓RR/↑TV: central cause (CNS disorder, opiate effect)
b. ↑RR/↑TV: increased work of breathing to overcome changes in lung compliance (pulmonary edema, pneumothorax, alveolar consolidation, ARDS) or need for greater levels of ventilation (CO2 production, sepsis, increased dead space)
c. ↑RR/⇔TV: other etiologies such as pain, bladder distention, and anxiety
2. Symmetry: The chest and abdomen should expand together with inspiration. Discordant movement may be seen during active exhalation, airway obstruction, and cervical spine paralysis with preserved diaphragm function. Pneumothorax, hemothorax, flail chest, splinting, and large bronchial obstructions can cause right/left asymmetry.
3. Accessory muscle use: Sternocleidomastoid and scalene muscle utilization suggests increased work of breathing and respiratory muscle fatigue/weakness. Firing of the external oblique muscles can signal active exhalation, a sensitive but not specific sign of respiratory distress.
4. Inspiratory/expiratory timing:
a. Long inspiratory time: upper airway or extrathoracic obstruction
b. Long expiratory time: intra-thoracic obstruction and/or bronchospasm
c. Inspiratory/expiratory pauses: sustained apnea necessitates intubation, but periodic breathing does not usually require intubation, though the cause should be investigated.
5. Auscultation/tactile exam:
a. Upper airway obstruction: Stridor, absent breath sounds, and lack of air movement from mouth/nose suggest upper airway obstruction (jaw thrust, chin lift, nasal airway may alleviate).
b. Other: Wheezing, rales, and absent breath sounds may indicate bronchospasm, pulmonary edema/consolidation, or pneumothorax, respectively.
E. Ventilation/Oxygenation Data
1. Arterial blood gas (ABG): Oxygen and carbon dioxide tensions and pH should be used to assess severity of disease and the success/failure of clinical interventions. It should not substitute for clinical judgment or delay critical interventions, but remains the most reliable test for oxygenation and ventilation.
2. Co-oximetry: Evaluation of arterial blood, or via noninvasive multiwavelength oximeters, can assay methemoglobinemia, carboxyhemoglobinemia, and desaturated blood.
3. Failed noninvasive positive pressure ventilation: Bi-level positive pressure ventilation (BiPAP) and continuous positive airway pressure ventilation (CPAP) can help avoid endotracheal intubation in patients with respiratory failure secondary to chronic obstructive pulmonary disease (COPD) and acute cardiogenic pulmonary edema. Lack of improvement justifies endotracheal intubation.
III. PREPARATION FOR PLACEMENT OF AN ADVANCED AIRWAY
A. Physical Exam/Patient History: A brief airway exam and history are necessary to minimize the chance of failing to ventilate/intubate, to predict the need for advanced intubation techniques, and to be aware of potential complications.
1. Airway anatomy: Less than three finger-breadths thyromental distance, small mouth opening, large incisors, limited ability to protrude the mandible, a large tongue, elevated Mallampati score, short neck, and limited cervical mobility may all contribute to difficult visualization of the glottis with laryngoscopy and should be checked.
2. Potential difficulty with mask ventilation: Facial hair, edentulousness, obesity, male gender, history of sleep apnea, and neck irradiation portend difficult mask ventilation.
3. Data on prior intubation attempts: If time permits, review old records for difficulty with prior intubation attempts and successful rescue techniques.
4. Allergies: Review for contraindications to the use of standard induction and maintenance drugs.
5. Coagulation status: Time permitting, a review of platelet count, PT/PTT, and current anticoagulation therapy is worthwhile, as profound anticoagulation may prohibit nasal airway manipulation given the risk of bleeding. The provider should be aware of potential for bleeding with multiple intubation attempts.
6. Neuromuscular status:
a. Patients with burns, crush injuries, prolonged immobility (>1–2 weeks), extensive upper motor neuron injury (such as debilitating stroke), denervation injuries, and myopathies are at risk of hyperkalemic arrest with the use of succinylcholine. Rocuronium is a viable alternative for intubation.
b. Cervical spine instability may require flexible fiberoptic or video laryngoscopic (e.g., GlideScope) intubation to minimize cervical manipulation.
c. Increased intracranial pressure (ICP), presence of intracranial aneurysms, intracranial hemorrhage, and symptoms of cerebral ischemia/infarct should be noted and may affect choice of induction medications.
7. Cardiovascular history: Angina/ischemia, arrhythmias, congestive heart failure, hypertension, and aneurysms should be noted given risk of cardiovascular collapse with common induction agents.
8. Aspiration risk: Recent gastric feeding, GERD, hemoptysis, emesis, bowel obstruction, obesity, pregnancy, and depressed mental status increase aspiration risk and may require rapid sequence intubation (RSI).
9. Hemodynamic stability: Note vasopressor requirements, work of breathing, blood pressure, heart rate, and oxygen saturation. Instability may require judicious use of induction agents.
B. Choice of Advanced Airway Placement Technique: Options include direct laryngoscopy, video-assisted laryngoscopy, blind naso-tracheal intubation, flexible fiberoptic intubation (nasal/oral), and/or supraglottic airway placement.
1. Direct laryngoscopy: performed with a laryngoscope and direct visualization of the glottis
a. Advantages: can be performed quickly with minimal equipment
b. Disadvantages: uncomfortable for awake patients and difficult with unfavorable airway anatomy or cervical spine instability requiring cervical spine fixation
2. Video-assisted laryngoscopy: Modified laryngoscopy blades with an anteriorly angled camera at the blade tip are commonly used in the setting of predicted or encountered difficult direct laryngoscopy due to anterior/superior larynx, small mouth opening, obesity/redundant laryngeal soft tissue, or limited cervical mobility. Available devices include the C-Mac (Karl Storz) and the GlideScope (Verathon).
a. Advantages: similar intubation mechanics to direct laryngoscopy with the advantage of an improved view of an anterior/superior glottis due to angled blade-tip camera
b. Disadvantages: being not always available in critical care units, cost, fragility, need for power source, limited portability, and unfamiliarity with device compared with direct laryngoscopy
3. Naso-tracheal Intubation: performed when the oral opening is insufficient for direct glottis visualization, in neck instability, and when access to a noninstrumented oral cavity is desired while maintaining an advanced airway
a. Advantages: more easily tolerated by minimally sedated patients when compared with oro-tracheal intubation. It can be performed on patients with unfavorable airway anatomy, in the sitting position to improve spontaneous respiratory mechanics/minimize aspiration, and without general anesthesia or paralytic agents.
b. Disadvantages: technically challenging, and spontaneous respiration must be present to guide blind placement via breath sounds. Placement under direct visualization with Magill forceps negates many advantages over oro-tracheal intubation. Contraindications include coagulopathy or planned anticoagulation/thrombolysis, nasal polyps, basilar skull fracture, and immunocompromise given increased risk of sinusitis. Endotracheal tube diameter may be limited given nasal passage size.
4. Flexible fiberoptic intubation: Insertion of an ETT over a flexible fiberscope with glottis visualization can be performed via the oral or nasal cavity.
a. Advantages: can intubate patients with unfavorable airway anatomy with minimal cervical manipulation. Fiberoptic visualization of the ETT tip upon airway exit can confirm accurate placement depth.
b. Disadvantages: technically difficult, equipment intensive, and visualization may be difficult with bleeding/excess secretions/distorted anatomy given decreased ability to suction or manipulate the airway
5. Supra-glottic airway: SGAs are the category of airway rescue devices that include the Laryngeal Mask Airway (LMA). As part of the ASA difficult airway algorithm, an SGA may be used as an emergency airway, especially as a bridge to endotracheal intubation. Some SGAs allow intubation through their lumens.
a. Advantages: rapid/easy placement in majority of patients
b. Disadvantages: not a long-term airway management strategy, decreased protection against aspiration, not tolerated by minimally sedated patients, risk of gastric insufflation with positive pressure ventilation if not placed appropriately
C. Monitors/Equipment: Essential monitors during acute airway management include pulse oximetry, blood pressure, and electrocardiography. All equipment must be ready for immediate use (a handy mnemonic is iSOAP).
1. Intravenous (IV) access: Adequate IV access should be available prior to intubation except in emergent cases such as cardiac arrest, which may necessitate intubation before IV access is obtained.
2. Suction: A functioning Yankauer or tonsil-tip suction device must be available.
3. Oxygen: An in-wall or tank oxygen (full) source and functioning bag-valve mask must be available for proper oxygenation.
4. Airway: A laryngoscope (Miller 2 or Macintosh 3 for adults, Miller 1 or Macintosh 2 for pediatrics), correctly sized endotracheal tube(s) (8.0 for men, 7.0 for women, see below for pediatrics) with stylet inserted and intact cuff must be available.
a. Pediatric ETT: Recent literature supports the use of cuffed endotracheal tubes when ETT diameter is >3.5 mm, and inflating the cuff until a leak is present at 20 cmH2O. If no cuff leak exists at 20 cmH2O, downsize the ETT diameter by 0.5 mm, and repeat leak test (Table 4.1).
| Endotracheal Tube Sizes | |
Age | Size (ID, mm)—Un-cuffed | Size (ID, mm)—Cuffed |
Preterm 1,000 g 1,000–2,500 g | 2.5 |
|
Neonate to 6 mo | 3.0 |
|
6 mo to 1 y | 3.0–3.5 | 3.0–3.5 |
1–2 y | 3.5–4.0 | 3.0–4.0 |
>2 y | 4.0–5.0 (Age in y + 16) / 4 | 3.5–4.5 (Age in y / 4) + 3 |
| Contents of Emergency Airway Kit | |
Airway Equipment | Pharmacologic Agents |
ETT with stylet (6.0, 7.0, 7.5 mm ID) | Propofol |
Laryngoscope handles (2—long, short) | Etomidate |
Laryngoscope blades (Mac 3, Miller 2) | Ketamine |
NPA | Midazolam |
OPA (No. 3, No. 5) | Fentanyl |
Bougie | Hydromorphone |
LMA (No. 4) | Rocuronium |
Syringes (3 cc, 5 cc, 10 cc, 30 cc) | Succinylcholine |
Tape | Phenylephrine |
End-tidal CO2 detector | Ephedrine |
IV catheters (14–20 gauge) | Glycopyrrolate |
Surgical lubricant | Esmolol |
5. Pharmacology: An induction agent, muscle relaxant, maintenance agent, vasopressor, vagolytic, and antihypertensive agent should be immediately available.
6. Table 4.2: Contents of Emergency Intubation Kit
V. INTUBATION TECHNIQUES: Successful intubation requires optimal patient positioning, adequate preoxygenation (if possible), and proper intubation technique.
A. Patient Positioning: Time to optimize position for intubation is well spent and should not be overlooked (Video 4.1: Patient Positioning).
1. Bed position in room: Move the head of the bed away from any walls, remove headboard, and bring the head of the patient to the edge of bed. If the headboard cannot be removed, place the patient diagonally in the bed for improved airway access.
2. Bed height: Elevate the bed so that the patient’s pharynx is between the operator’s umbilicus and xyphoid process. Consider slight reverse Trendelenberg position to minimize aspiration risk.
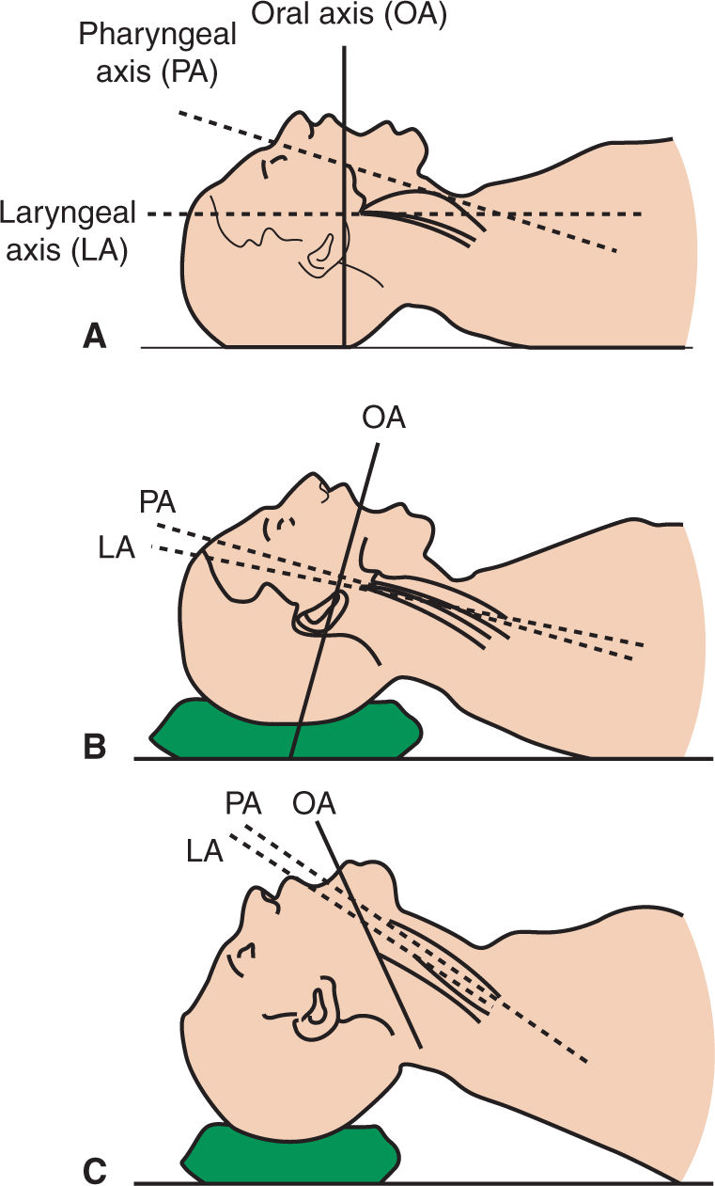
3. Align pharyngeal, laryngeal, and oral axes: In the supine position, the laryngeal, pharyngeal, and oral axes are not parallel (Fig. 4.1a), inhibiting glottis visualization. Creating the “sniffing position” with neck flexion via blankets under the occiput (Fig. 4.1b) and head extension on the atlanto-axial joint (Fig. 4.1c) will align the three axes. Fig. 4.1c illustrates the ideal position where the laryngeal, pharyngeal, and oral axes are nearly parallel.
4. Trauma patients: All trauma patients who have not received definitive cervical spine clearance via NEXUS or Canadian C-spine rules, CT, or MRI (if obtunded), should be assumed to have a cervical spine injury. During airway management, the patient should remain in a c-collar or an assistant should hold the patient’s neck/head in the neutral position. Awake fiberoptic intubation should be used for alert/awake patients in nonemergent cases, while direct orotracheal intubation with neck stabilization is appropriate in all other cases. Note that bag-mask ventilation is the time of greatest cervical manipulation.
B. Pre-Oxygenation: Replacement of functional residual capacity (FRC) nitrogen with oxygen is critical prior to intubation to maximize tolerated apnea time. This is especially relevant with obese patients, who should be preoxygenated to an end-tidal oxygen level >85%.
1. Awake/alert patient: Tightly seal bag-valve mask over nose and mouth, provide 100% oxygen at high flows >10 L/min, encourage tidal volume breathing for 3 minutes, or vital capacity breathing if time limited, and use gentle chin-lift/jaw thrust maneuvers as needed to ensure airway patency. Postinduction, maintain airway seal and patency during the time between induction and intubation, as apneic oxygenation can maintain oxygenation.
2. Obtunded patient: Without adequate respiratory effort, 8 to 10 breaths per minute of positive pressure ventilation/support with a bag-valve mask at 100% oxygen is required for preoxygenation. Airway adjuncts to ensure airway patency such as an oropharyngeal or nasopharyngeal airway may be required if bag-mask ventilation with head positioning and chin-lift/jaw thrust maneuvers is ineffective.
a. Oropharyngeal airway (OPA): Provided in three adult sizes (Sizes 3, 4, 5–80, 90, 100 mm, respectively), which is the distance from the tip to flange. Proper size can be estimated by measuring distance from ear lobe to the ipsilateral corner of the lip. The distal tip is inserted facing upward against the hard palate and then rotated 180 degrees to advance into posterior pharynx. An OPA that is too short may cause obstruction by pressing the tongue into the posterior pharynx, while an OPA that is too long may push the epiglottis against the glottis opening. An OPA may cause laryngospasm or emesis in a conscious or semiconscious patient.
b. Nasopharyngeal airway (NPA): Optimal for use in obstructed patients with intact oropharyngeal reflexes or minimal mouth opening when bag-mask ventilation is inadequate. NPAs are sized for adults by internal diameter (6–9 mm), should be inserted into the naris parallel to the hard palate after lubrication, and advanced until the flange rests on the outer naris. Use the largest diameter that will fit into the naris with minimal resistance. Bleeding tendency is a relative contraindication to NPA placement while basilar skull fractures are a more absolute contraindication to NPA placement. NPAs are less likely to induce vomiting and are better tolerated than OPAs in awake/minimally obtunded patients.
C. Orotracheal Intubation: Direct laryngoscopy, video-assisted laryngoscopy, and flexible fiberoptic intubation are common methods for oral ETT placement.
1. The laryngoscope: Direct visualization of the glottis can be achieved using a laryngoscope with either a Macintosh or Miller blade. Some laryngoscopes have the light emitted from a bulb on the blade; some fiberoptic systems have the light source in the handle, with light carried to the blade tip. Nonfiberoptic handles and blades are not compatible with fiberobtic handles and blades. It is critical to ensure the system works (Fig. 4.2).
a. Laryngoscope handle: provides a place to apply a firm grip with the left hand.
b. Macintosh blade: a curved blade that is inserted into the vallecula (the space between the base of the tongue and the pharyngeal surface of the epiglottis). Upward pressure against the hyoepiglottic ligament elevates the epiglottis, exposing the glottis. Sizes range from No. 0 to No. 4, with No. 3 as the most commonly used blade in adults. Its deep flange provides more room for ETT passage when compared with a Miller blade (Video 4.2: Direct Laryngoscopy).
c. Miller blade: A straight blade whose tip is inserted underneath the laryngeal surface of the epiglottis and lifted to expose the glottis. The smaller flange provides less space for ETT placement. Sizes range from No. 0 to No. 3, with No. 2 being the most common size for adults.

FIGURE 4.2 Laryngoscopes (Clockwise from bottom left: GlideScope, C-Mac, Miller 2, Macintosh 3, laryngoscope handle)






Full access? Get Clinical Tree


