Albumin >2.5 g/dl
Albumin <2.5 g/dl
Total cortisol (μg/dl [nmol/l])
Baseline
15 (410)
10 (275)
Stimulated
20 (550)
15 (410)
Free cortisol (μg/dl [nmol/l])
Baseline
1.8 (50)
1.8 (50)
Stimulated
3.0 (85)
3.0 (85)
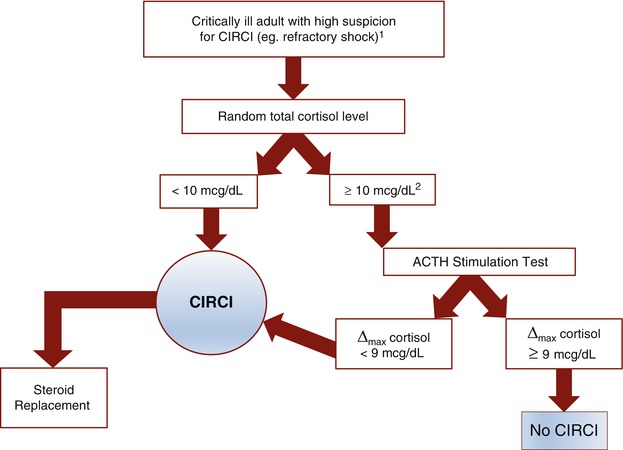
Fig. 49.1
Decision Tree for Investigation of CIRCI in Critically Ill Adults. CIRCI critical illness-related corticosteroid insufficiency,;ACTH adrenocorticotropic hormone, Δ max maximum change in cortisol level after ACTH stimulation. 1Routine screening for all patients with septic shock is not recommended. 2There is no firm cutoff in random cortisol above which CIRCI is ruled out, but some authors have suggested that a random cortisol of >34 mcg/dL rules out significant CIRCI, and thus ACTH stimulation would not be performed (see Cooper and Stewart [15])
In patients with septic shock, the routine use of either random serum cortisol or ACTH stimulation testing are not recommended for broad screening for hydrocortisone replacement therapy [5, 16]. (See “Steroid replacement in septic shock” below.)
Steroid Replacement Strategies
Choice of Steroid
Hydrocortisone is considered the steroid of choice for replacement therapy in patients with acute adrenal crisis and with CIRCI including septic shock with persistent hypotension despite fluid resuscitation [16]. There is no evidence to recommend routine mineralocorticoid (fludrocortisone) replacement for patients in the ICU, unless they have known or suspected primary adrenal insufficiency. Even in Addisonian crisis, hydrocortisone along with saline resuscitation is probably sufficient for initial treatment in the acute setting because hydrocortisone does have some mineralocorticoid activity. A study evaluating hydrocortisone alone vs. hydrocortisone plus fludrocortisone in patients with septic shock failed to show any significant differences in outcomes with the addition of the mineralocorticoid [17].
Steroid administration for treatment of presumed adrenal crisis should never be delayed in order to perform random cortisol and ACTH stimulation testing. Dexamethasone may be useful in such patients because, unlike hydrocortisone, it does not interfere with measurements of serum cortisol. Dexamethasone can cause long-term suppression of the HPA axis, however, and thus it is not generally recommended for ongoing steroid replacement [8].
Dose and Duration
In suspected acute adrenal crisis, an initial dose of 100 mg hydrocortisone IV followed by 100–200 mg daily is generally adequate [1, 18]. For CIRCI in the setting of severe sepsis and septic shock, 200 mg of hydrocortisone divided into 3–4 intermittent doses daily has been recommended [16]. Hydrocortisone is typically not tapered until patients are no longer requiring vasopressors. Tapering can occur over several days to prevent rebound hypotension and adverse immunologic effects. Discontinuation of steroids after tapering may be contraindicated in patients with adrenal crisis not consistent with CIRCI as they may require ongoing low-dose corticosteroid replacement.
Concurrent Fluid Management
In primary adrenal insufficiency, patients have urinary salt-wasting with subsequent volume depletion that should be replaced using 0.9 % saline. In secondary adrenal insufficiency, patients do not exhibit salt-wasting, but they do have decreased vascular tone resulting in hypotension, and thus isotonic fluid resuscitation is also generally necessary in the acute setting. Dextrose can be administered concurrently in hypoglycemic patients.
Additional Testing
Because CIRCI is dynamic, generally reversible, and can occur at any time during a patient’s ICU stay, routine follow-up testing after treatment of acute critical illness is not generally necessary. However, a small number of patients with CIRCI may develop prolonged adrenal dysfunction due to adrenal infarction or hemorrhage as seen with sepsis or coagulopathy, or injury from medication [5, 19]. Such patients warrant close follow-up and additional testing in the outpatient setting.
There are no guidelines to suggest routine adrenal or brain imaging for CIRCI. However, if infection, bleeding, tumor, or other pathologic disease of the adrenals is specifically suspected, then abdominal CT scanning may be indicated [18]. Additionally, MRI of the pituitary and hypothalamus may be useful in evaluating patients with probable secondary adrenal insufficiency not consistent with CIRCI, and without other obvious causes. Unless there is concern for a more emergent diagnosis, this may be deferred to the outpatient setting if adrenal insufficiency persists.
Evidence Contour
Steroid Replacement in Septic Shock
In 2002, a large prospective study demonstrated that 7 days or hydrocortisone and fludrocortisone reduced the 28-day mortality for patients with septic shock [20]. However, the subsequent Corticosteroid Therapy in Septic Shock (CORTICUS) trial failed to replicate any mortality benefit after treatment with hydrocortisone [21]. Patients receiving hydrocortisone did recover from shock more quickly, regardless of results of ACTH stimulation testing, but had a trend toward increased hospital-acquired infections. Furthermore, an observational study by the Surviving Sepsis Campaign showed an increase in hospital mortality in vasopressor-dependent patients receiving low-dose corticosteroid therapy [22].
Systematic reviews and meta-analyses have attempted to resolve the conflicting evidence. Several such studies have indicated that low dose corticosteroid therapy aids in reversal of shock, and thus patients who are vasopressor-dependent despite adequate fluid resuscitation may benefit from corticosteroid therapy [23–27]. However, ACTH stimulation testing has not been shown to accurately discriminate which patients with septic shock will benefit from steroid replacement [8, 16, 26].
Based on this body of evidence, the Surviving Sepsis Campaign no longer recommends routine use of steroid replacement therapy as part of its sepsis care bundles [28]. However, the most recent Surviving Sepsis Guidelines include a Grade 2C (weak) recommendation to consider steroid therapy in patients with severe, persistent, vasopressor-dependent septic shock [16].
ACTH Stimulation Test: Low Dose Versus High Dose
Administration of 250 mcg of ACTH is commonly used in ACTH stimulation testing. This “high dose” testing uses supraphysiologic dosing of ACTH, and thus a “low dose” test using only 1 mcg of ACTH has been used as an alternative. The low dose test has better sensitivity, is less expensive, and has been shown in at least one study to better delineate groups of patients with relative adrenal insufficiency in septic shock [4]. However, there is the practical concern of how to accurately dilute the 250 mcg dose, as well as concerns that much of the ACTH dose may bind to injection tubing leading to unknown dose delivery [18]. Furthermore, the high dose ACTH test is better validated, having been used in numerous studies in ICU patients [8, 20, 22, 23, 29] and therefore it remains the favored test in critically ill patients.
Role of Salivary Cortisol Testing
Salivary cortisol measurements have been used as a surrogate marker of free cortisol in the diagnosis of adrenal insufficiency [30–32], but salivary cortisol has not been validated as a standalone diagnostic test in adults with suspected CIRCI. A recent study in neurosurgical ICU patients showed a lack of diurnal variation in salivary cortisol production, similar to that seen with serum cortisol, but the authors described challenges in collecting saliva from intubated patients due to decreased salivary flow and dry oral mucosa, medication effects, fluid imbalances, mucosal breakdown, and contamination with blood [33].
Role of Etomidate and Opiates in Development of Adrenal Insufficiency
Etomidate is an anesthetic agent commonly used during rapid sequence intubation in critically ill patients. Etomidate can cause inhibition of adrenal 11-β-hydroxylase, however, and thus has been implicated in adrenal insufficiency. In the CORTICUS trial, patients who received etomidate were less likely to have a significant increase in cortisol after ACTH, and they had decreased survival at 28 days [21]. In the retrospective CORTICUS study, etomidate administration in critically ill patients was associated with a worse prognosis in patients not treated with steroids [29]. Etomidate has other benefits including a very short duration of action, decreased respiratory depression and less hypotension [34]. The balance of risks and benefits using etomidate for induction of anesthesia during intubation remains unclear in the context of adrenal insufficiency.
Related posts:






Full access? Get Clinical Tree


