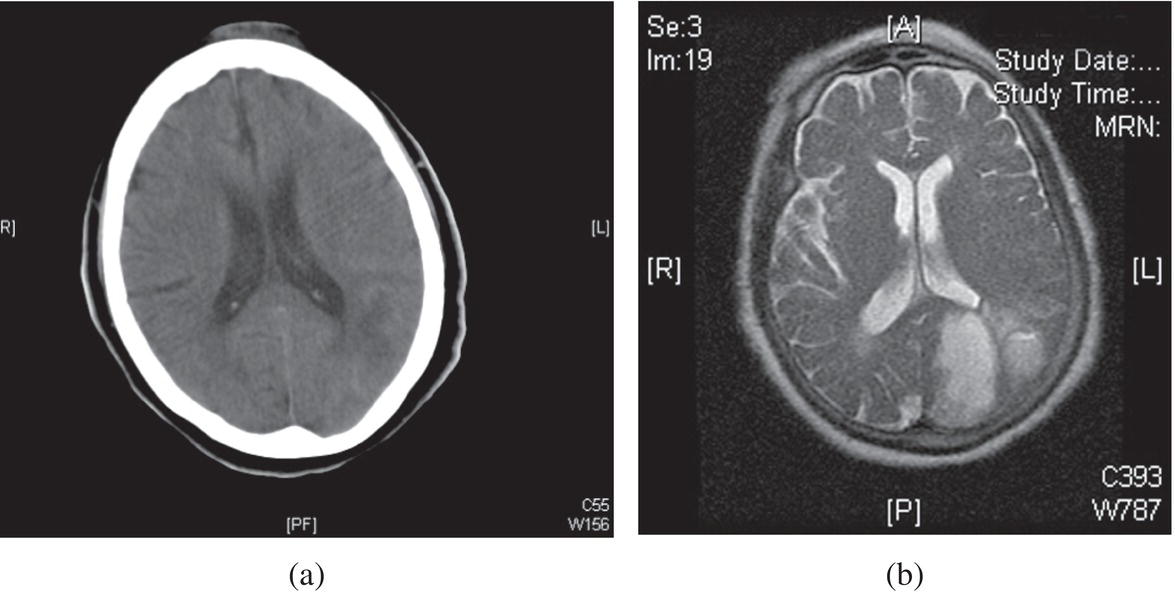
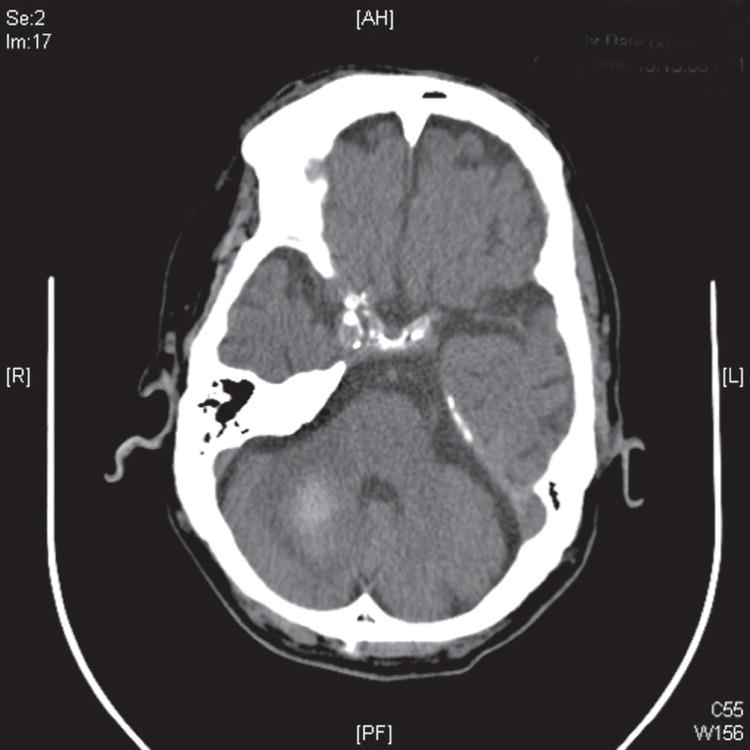
John Bedolla1 and Jesse M. Pines2,3 1 Department of Surgery and Perioperative Care, Dell Medical School, University of Texas at Austin, Austin, TX, USA 2 US Acute Care Solutions, Canton, OH, USA 3 Department of Emergency Medicine, Drexel University, Philadelphia, PA, USA Stroke is the leading cause of disability and the third‐leading cause of death in the United States. Rapid bedside and radiological evaluation of cases of suspected acute stroke within 4.5–6 hours of symptom onset are critical in the assessment of patients potentially eligible for intravenous (IV) and intra‐arterial thrombolysis. In acute ischemic stroke (Figure 47.1), the central event is an acute vascular occlusion; however, 15% of strokes are hemorrhagic (Figure 47.2). Hemorrhagic strokes do not benefit from thrombolysis, as it can worsen bleeding and increase mortality. While this chapter focuses on the diagnosis of stroke, it is important to consider why the diagnosis of stroke is clinically important. Importantly, when the correct diagnosis of stroke is made in a timely way, early interventions such as tissue plasminogen activator (tPA) and endovascular treatment (i.e., mechanical thrombectomy) have been shown to improve outcomes.1 The approach to diagnostic imaging depends on patient characteristics, time since symptoms onset, and local availability of imaging and stroke expertise. Traditionally, noncontrast head computed tomography (NCHCT) has been the first imaging modality in acute stroke in the emergency department (ED) (Figure 47.1). NCHCT can rule out hemorrhagic stroke, completed stroke, and also exclude other potential causes of acute neurological symptoms. NCHCT is widely available, easier, and faster to perform with shorter scan times and fewer patient exclusions/contraindications, has lower cost compared to MRI, and is a cost‐effective strategy.2 In cases where a large vessel occlusion (LVO) is suggested on exam, computed tomography angiogram (CTA) head and neck can also be performed to demonstrate large clots that are best treated with IV or arterial tPA or mechanical clot retrieval. A LVO is defined as the occlusion of the internal carotid artery and of the proximal segments (M1, M2) of the middle cerebral artery. In cases where the deficit is equivocal or the timing of last known normal is uncertain more advanced imaging technique, multimodal magnetic resonance imaging (MRI) with diffusion‐weighted imaging (dwMRI) and perfusion MRI, or computed tomography perfusion (CTP) can be performed after computed tomography (CT) because these advanced imaging methods are considered a more accurate diagnostic test for demonstrating acute ischemia. CTP is particularly useful in selecting patients amenable to mechanical thrombectomy, particularly those within 24 hours of symptoms including those with unknown symptoms onset (wake‐up strokes). Diffusion‐weighted magnetic resonance imaging (dwMRI) is sensitive for acute ischemia, however the primary clinical concerns regarding the use of dwMRI as a solitary test are (i) reduced ability to detect intracranial hemorrhage in the setting of acute stroke, (ii) less clinical access to potentially unstable patients, (iii) longer testing times, and (iv) poor availability of rapid MRI. Figure 47.1 Noncontrast head CT showing ischemic stroke in the left posterior cerebral artery region (a), confirmed on MRI (b). Figure 47.2 Noncontrast head CT showing a right cerebellar hemorrhage. What is the sensitivity of diagnostic modalities (head CT and MRI) in acute stroke, and does MRI miss acute intracranial hemorrhages? A study comparing NCHCT to dwMRI included articles in which both head CT and dwMRI were performed within 6–7 hours of the onset of clinical symptoms.3 A total of eight studies and 909 patients were included. The largest included study was a retrospective review of patients seen in the ED for signs and symptoms of acute stroke.4 Of 691 patients, 509 had a NCHCT and 122 had dwMRI within 6 hours of ED arrival. They used a primary discharge diagnosis of stroke as the criterion standard. The study reported a sensitivity of NCHCT of 40% and of dwMRI of 97%; the specificity was 92% for both modalities. The positive predictive value (PPV) of head CT and dwMRI were each 96%. The negative predictive value (NPV) were 23% for head CT and 77% for dwMRI. The authors went on to review seven smaller studies (ranging in sample size from 17 to 54), most with considerable methodological issues including variable inclusion criteria, variable criterion standards for stroke, delays between head CT and dwMRI, and variable blinding of reviewers.5–11 They then combined data from all eight studies (despite variable inclusion criteria and heterogeneity of the studies) to calculate a sensitivity, specificity, PPV, and NPV for each modality. For dwMRI, their calculated sensitivity was 97% (confidence interval [CI] 94–98%) and their specificity was 100% (CI 88–100%), with a PPV of 100% (CI 98–100%) and a NPV of 91% (CI 75–98%). The sensitivity of head CT was 47 % (CI 43–51%), specificity was 93% (CI 85–97%), the PPV was 97% (CI 94–99%), and the NPV was 23% (CI 19–28%). In this systematic review the authors excluded four studies from the pooled diagnostic test accuracy calculations because these studies did not have patients without a stroke or required a negative CT as part of the original studies, limiting the calculations. A single center prospective study compared dwMRI to NCHCT in the ED in patients with suspected stroke.12 MRI detected acute ischemic stroke in 164/356 patients (46%, CI 41–51%) compared with CT in 35/356 patients (10%, CI 7–14%), p
Chapter 47
Acute Stroke
Background
Clinical question





Full access? Get Clinical Tree


