Gastrointestinal origin
Appendicitis
Mesenteric adenitis
Intussusception
Terminal ileitis
Cecal diverticulitis
Epiploic appendagitis
Typhlitis
Inflammatory bowel disease
Constipation
Urogenital
Ureteral stone
Urinary tract infection
Gynecologic
Tubo-ovarian abscess
Ovarian torsion
Ectopic pregnancy
Hemorrhagic ovarian cyst of corpus luteum remnants
Ruptured ovarian cyst
Pelvic inflammatory disease
Perforated duodenal ulcer with retroperitoneal extension (“Valentino’s Appendix”)
Pancreatic abscess with retroperitoneal extension
Symptom | Points |
Migratory right iliac fossa pain Nausea/vomiting | 2 1 |
Sign | |
Right lower quadrant pain Rebound tenderness Fever Rovsign’s sign | 2 1 1 1 |
Laboratory value | |
Leukocytosis | 2 |
Imaging
As described previously, a careful history and physical exam in combination with isolated leukocytosis will often provide the diagnosis of AA. Prior to the omnipresence of the CT scanner, a 20% negative appendectomy rate was considered an acceptable variance. A higher number indicated hasty procession to the operating room, while a lower number led to the concern that cases were being missed. By 1997, the frequent use of CT scanning had reduced the negative appendectomy rate to 15%, with numbers continuing to decrease to 10% with the use helical or multidetector CT scanners [8, 9]. Since the potential postoperative complications for a negative appendectomy are the same as for appendicitis, the benefits of obtaining a CT scan should be weighed against the risks. While a scan increases cost, radiation exposure, and potential time prior to proceeding to the operating room, it can also provide valuable information for plan of care. The presence of a phlegmon, predominant inflammation of the terminal ileum or cecum, identification of other pathology, or nonspecific findings in a high-risk patient can all save a patient from an unnecessary or dangerous operation and guide alternate therapy.
Acute appendicitis can often be readily identified on the different variations of abdomen/pelvis CTs performed with a sensitivity and specificity of approximately 94% [10]. Non-contrast (both intravenous and oral) CTs, those with both types of contrast or with oral and rectal contrast may all be helpful in making the diagnosis. Findings include an enlarged appendix, fat stranding around the tip or in the right lower quadrant, the presence of an appendicolith, non-filling of the appendix with oral or rectal contrast, or a phlegmon with or without abscess (see Figs. 25.1–25.3). Patients with little visceral adiposity make the diagnosis slightly more difficult, as there are reduced fat planes to highlight inflammation. Enlarged fallopian tubes or adnexal pathology in the female patient may also be difficult to distinguish from appendiceal inflammation on CT scan.


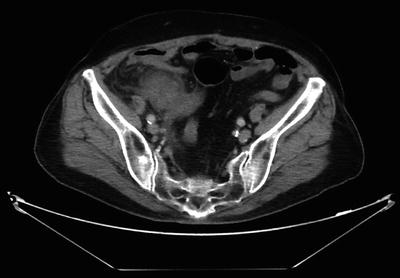
Fig. 25.1
Coronal CT image of acute non-perforated appendicitis. A dilated tubular structure (arrow) in the right lower quadrant is demonstrated. Inflamed periappendiceal fat can also be appreciated by darkening of the fat plane around the structure
Fig. 25.2
Axial CT image of acute appendicitis with appendicolith. The appendicolith (arrow) is noted as a white structure within the lumen of the mid-portion of the appendix
Fig. 25.3
Axial CT image of perforated appendicitis with phlegmon. Dense mass is noted with no definite separation of cecum from appendix. Generalized inflammation is noted in the right lower quadrant
Ultrasonography or magnetic resonance imaging (MRI) may be obtained for patients in whom radiation exposure should be limited. Ultrasound (US) is often used for the pediatric population, as it can be an extension of the exam and does not require sedation or travel out of the emergency room. The inflamed appendix on US appears as an incompressible, blind-ended, tubular structure with diameter greater than 6–7 mm. With graded compression, differentiation between normal loops of bowel and the appendix can be achieved [11]. Sensitivity and specificity of US for AA is approximately 83 and 93% [10]. MRI is often utilized for the pregnancy patient, as excellent imaging can be obtained with no radiation exposure. Contrast agents should not be administered. Although MRI is costly and may not be widely available, the risk of unnecessary laparoscopy or missed appendicitis in the pregnant patient can increase preterm contractions and fetal mortality. The sensitivity and specificity of MRI for AA in this patient population is approximately 100% and 93%, respectively [12].
Plain abdominal films are often obtained initially when in the emergency room, but these provide little information indicative of appendicitis unless an appendicolith is present, and are primarily used to rule-out more acute disease processes such as a perforated viscus or complete bowel obstruction.
Surgical Management
Most cases of AA will present in an uncomplicated manner and often proceed to the operating room with little deliberation regarding management. This holds true for the patient with little comorbidity and with suspected non-perforated appendicitis. Although a prompt operation is considered standard procedure, cases in select patient populations can often be delayed up to 12 h with no increase in morbidity [13]. In a large retrospective observational dataset, the risk of rupture for appendicitis was not increased with a delay of up to 24 h from hospital admission to operation[14]. A 6% increase in rupture rate was encountered if a delay over 36 h was noted. Again, the pathology of ruptured versus non-ruptured appendicitis has been debated, with less emphasis given to early operation for the prevention of rupture. A significant delay in surgery should still be avoided, however, as an expedited operation can reduce the suffering of the patient, in addition to reducing hospital cost by an extended length of stay. Preoperative preparation should be straightforward, with initiation of intravenous fluids, and demonstration of a negative pregnancy test for women of child-bearing age. Deep venous thrombosis prophylaxis and antibiotic prophylaxis should be initiated prior to surgery as indicated by standard guidelines [15].
Postoperative morbidity associated with appendectomy ranges from 10 to 20% for non-perforated appendicitis versus 30% for those with perforation. Most of these complications are infectious in nature [16]. Mortality for appendectomy is low, with a rate of 0.07–0.7% without perforation, and 0.5–2.4% with perforation [3, 17]. The mortality rate increases with comorbidities including cardiac risk factors, pulmonary disease, and morbid obesity. Age also increases mortality, with rates of 2.5% for patients in their 70s, 6.8% in their 80s, and 16.4% for those 90 years of age and older [18].
Laparoscopic Versus Open Technique
Standard open surgical technique for appendectomy includes an approximately 5 cm incision in the right lower quadrant through which the peritoneum is reached via a muscle slitting technique. The appendix and mesoappendix can then be suture ligated and divided, and the wound closed in layers after irrigation. With the availability and mastery of laparoscopic techniques, as well as the advancing rate of obesity of the population, this open technique is often considered a secondary approach. The laparoscopic approach is usually performed using three ports placed on the left side of the patient, with left arm tucked for better movement of the surgeon and assistant on the same side (see Fig. 25.4). A Foley catheter is placed to decompress the bladder as suprapubic ports are often placed. The appendix can be divided with an endovascular stapling device or with suture ligation. The mesoappendix may also be divided using a stapler, or various cautery devices. In theory, the laparoscopic approach provides better visualization of the abdomen when other pathology may be suspected. There is also the bias towards laparoscopy due to potential reduction of pain, infection, or resumption of diet.
Fig. 25.4
Operative configuration for laparoscopic appendectomy. Possible operating room configuration for laparoscopic appendectomy is illustrated. Both surgeon and assistant stand on the patient’s left for better ergonomic approach to the right lower quadrant of the abdomen. The patient’s left arm should therefore be tucked to prevent excessive extension at patient’s shoulder. Black X shapes demonstrate common port site placement for appendectomy, although additional or replaced ports may be placed as illustrated by the white plus shapes
The specific merits of a laparoscopic appendectomy (LA) over open appendectomy (OA) have been debated, however, particularly for obese patients or those with complicated AA. Initial series of comparative studies demonstrated possible faster recovery, earlier resumption of diet, and improved wound healing with LA versus OA. Other studies during the same time demonstrated no benefit. Most of these publications were small, and were thus underpowered. A meta-analysis performed in 2010 included 44 studies, pooling the results of appendectomy on 5,292 patients [19]. The only significant differences in outcome between the two techniques included slightly (8.67 min) longer operative time and slightly shorter length of hospital stay (0.6 days) for laparoscopic cases. Further, a Cochrane review in 2010 reviewed 56 studies [20]. This likewise demonstrated longer operative time (10 min) and shorter length of stay (1 day) with LA. These patients also had a lower subjective pain scale on postoperative day 1. While operative costs were significantly higher for laparoscopic cases, the out-of-hospital costs were lower.
The National Surgical Quality Improvement Program (NSQIP) provides a large standardized dataset of sampled surgical outcomes that can be accessed on a continuous basis. Based on a 2008 query that included 32,683 patients, 76.4% of appendectomies were performed laparoscopically [21]. Patients who underwent an open technique were statistically older, with increased comorbidities. On multivariate analysis, patients with LA had a decreased likelihood of developing any morbidity postoperatively, none of which were considered serious. Caution must be taken when interpreting this data, however, as causality cannot be ascertained. Those patients with comorbidities may have had an open procedure performed due to perceived decrease in operative time, inability to tolerate pneumoperitoneum due to cardiopulmonary disease, or other concerns by the surgeon.
Further query of the NSQIP dataset delineates more specific outcomes for appendectomy, particularly infection risk [22]. When adjusted for body mass index (BMI), sepsis, and operative time, wound infection had a risk reduction of 63% with LA. When adjusted for confounders, however, a 44% higher risk of organ space infection was noted for LA. Patients with wound class II, III, and IV had higher risk of organ space infection with a laparoscopic approach. In summary, the overall risk of complications was lower for LA, mostly due to a lower rate of wound infections; however, those patients with a greater degree of contamination had a higher risk of deep space infection postoperatively when LA was performed. This opposes the conventional wisdom that the laparoscopic approach affords a more thorough ability to washout the abdomen. The suction/irrigator may simply spread bacteria throughout the pelvis to a greater degree than with the limited view and dissection of the open technique.
Often surgeons advocate for the laparoscopic approach when operating on the obese patient. Less soft tissue dissection and greater visibility are often cited. Obese patients may also present a problem for the laparoscopic approach, however, due to diminished ability to ventilate during pneumoperitoneum and difficulty placing trocars or achieving appropriate angles for dissection due to soft tissue thickness. While reports of diminished wound infections in obese patients are noted in smaller reports, larger series comparing open to laparoscopic appendectomy demonstrate no difference in postoperative complications for these patients [23].
In summary, in a setting where basic laparoscopic expertise and equipment are available, LA has various slight advantages over OA, though some effects are small and of limited clinical significance. Women should be considered for a laparoscopic approach, as other adnexal pathology can be determined at operation. Young, employed, and more ambulatory patients also demonstrate added benefit from LA over OA, particularly in terms of resumption of activity and work.
Appendiceal Phlegmon or Abscess
Patients outside of the young, healthy demographic or who complain of prolonged periods of pain, may in fact present with an appendiceal phlegmon or abscess instead of simply suppurative appendicitis. A phlegmon consists of a mass of dense inflammatory tissue, often consisting of periappendiceal fat, but which may also include the cecum and/or terminal ileum. When encountered in the operating room, a phlegmon can significantly increase the difficulty of dissection, resulting in injury to adjacent tissues, or necessitating cecectomy or right hemicolectomy in order to achieve margins of resection that are not inflamed. An appendiceal abscess likewise represents a process which has walled itself off and clinically may result in less peritonism or systemic sequelae. In these cases, the acute process has already run its course, and secondary stages of inflammation with fibrosis have begun. Once inflammation has progressed to this stage, operative intervention becomes more dangerous, with risks of complications threefold higher in surgical versus nonsurgical management of cases of appendiceal phlegmon [24].
Overall, 2–6% of patients with AA will have some sort of inflammatory mass, and of those with an abscess, 20% will require drainage [25]. Of those requiring drainage, 2–6% will need to be approached in the operating room, due to inability to either access or adequately drain the collection percutaneously [26]. The early case series of patients treated in this manner were primarily pediatric, as the clinical presentation of symptoms was often late and surgical intervention less desirable. These patients often underwent treatment with antibiotics, with or without drainage, with planned interval appendectomy often 6–12 weeks later. Delayed operation was favored as the majority of the inflammation had subsided by this point, making operative intervention safer with reduced risk to adjacent organs [27, 28]. With success of this approach in the pediatric population, the adult population was treated similarly. Overall, conservative management of an appendiceal phlegmon was successful (i.e., did not require operative intervention) 76–97% of the time [29–32]. One of the larger studies comparing patients who underwent immediate surgery versus percutaneous drainage and interval appendectomy for AA with periappendiceal abscess included 104 patients. Patients who underwent immediate operation had a significantly higher rate of complications at initial hospitalization (58% versus 15%, p < 0.001). This group likewise had longer length of hospital stay [33].
Interval Appendectomy
The necessity of interval appendectomy after successful treatment with percutaneous drainage and antibiotics has been recently debated. Although expeditious surgical treatment has been considered the treatment of choice, the concept of delaying operation until inflammation has subsided has been proposed since the early 1900s [34]. Interval appendectomy is often recommended based on risk of subsequent AA or of risk of missing an incidental malignancy. A large retrospective study demonstrated a total recurrence rate of 14.6% in patients treated with antibiotics alone for phlegmon [35]. The majority of these recurrences occur within 3–6 months [31, 36, 37]. At this rate, interval appendectomy at 12 weeks would only prevent half of the potential recurrences. The recurrences that do occur have a relatively mild clinical course [24, 38]. There are likewise risks to operating in this setting, with complication rates for interval appendectomy ranging from 4 to 17% [29, 30]. This information has led some practitioners to approach an interval appendectomy with more expectant management depending on patient preference and perceived risk of malignancy [39].
Related posts:






Full access? Get Clinical Tree


