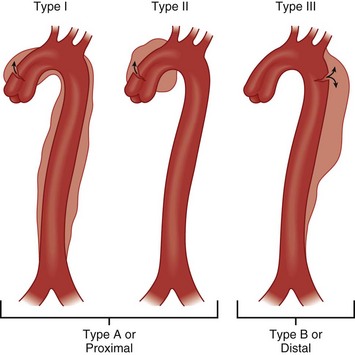
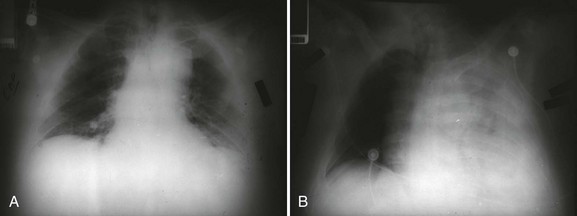
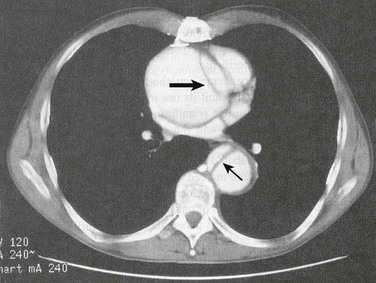
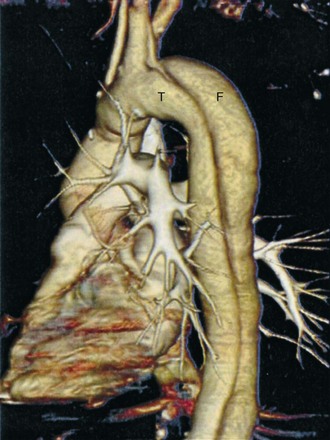
Chapter33 Thoracic aortic dissection (TAD) occurs with communication between the thoracic aorta lumen and wall with a separation of the thoracic aortic wall layers. Thoracic aortic dissection is to be contrasted with thoracic aortic aneurysm (TAA), which is defined as dilation of the thoracic aorta to a diameter of ≥1.5 times normal. Thoracic aortic aneurysm is a risk factor for TAD. Thoracic aortic aneurysm, although an important morbidity that may be associated with acute catastrophic leakage and death, is in and of itself not the acute emergency that is signified by a TAD. The international registry of acute aortic dissection reported an overall mortality of 27.4% with this condition. Surgical mortality was 26% for proximal (type A dissection) versus 58% for medical management and for distal (type B dissection), with 10.7% for medical management and 31% for surgical management.1 In 1819, Laenec introduced “aortic dissection” into the medical literature when he described an intimal tear distal to the aortic valve associated with a longitudinal space in the aortic wall postmortem.2 An autopsy report in 1760 described aortic dissection and pericardial tamponade as the causes of death of King George II.3 In 1863, Peacock reported a summary of findings in 80 patients with aortic dissection and classified the disease into three stages: intimal tear, propagation of the dissection with the potential for rupture, and recanalization of the lumen.4 In 1896, Marfan described the aortic connective tissue abnormality now known to be associated with this entity.5 In 1955, DeBakey treated a descending thoracic aortic dissection with resection and reapproximation of dissected layers with graph interposition.6 In 1963, DeBakey and colleagues repaired an ascending aortic dissection complicated by aortic valvular insufficiency.7 The thoracic aorta is divided anatomically into the ascending portion, the transverse portion, and the descending portion.8 The ascending aorta has two sections, the aortic root (valvular annulus and sinuses) and the tubular portion extending to the origin of the innominate artery. The transverse portion of the aorta is a short segment, and the brachiocephalic arteries come off this portion of the aorta. The descending thoracic aorta begins immediately distal to the left subclavian artery and extends to the diaphragm. The anatomic location of TAD has important clinical and prognostic implications. The most commonly used classification scheme for TAD is the Stanford System (Fig. 33.1), which has mostly replaced the first classification system, the DeBakey System (see Fig. 33.1). An advantage of the DeBakey System is that it does distinguish between dissections that are confined only to the ascending aorta (DeBakey type 2) and dissections that involve the entire aorta (DeBakey type 1). Using the Stanford System, which is more simplistic, any involvement of the ascending aorta classifies the dissection as a Stanford A, whereas lack of ascending aorta involvement classifies the dissection as a Stanford type B. Multiple risk factors for TAD have been identified.8 Men are at greater risk for developing TAD than women; approximately two thirds of patients with TAD are male.9 The sex distribution is consistent across different classifications of aortic dissection. Women with TAD are more likely than men to have a history of hypertension. Women are older at the time of diagnosis of TAD when compared to men. The average age at diagnosis of TAD is 65 years and is younger for type A TAD than for type B TAD.8 Specific risk factors for TAD are shown in Table 33.1. It is thought that the higher the blood pressure, the greater the probability of aortic dissection. In the presence of coarctation of the aorta, acute dissection typically occurs proximally rather than distal to the coarctation. The majority of patients with aortic dissection have hypertensive disease at the time of diagnosis.10 It is thought that blood pressure control decreases the occurrence of aortic dissection. However, hypertension is not thought to be the sole cause of dissection in a given patient. Many think that pregnancy is an independent risk factor for aortic dissection, although analysis of the available data and the conclusions from these data is hampered by the small number of patients affected and coexisting additional predisposing factors such as hypertension.11–13 In addition to blunt trauma, thoracic aortic dissection may be induced following establishing antegrade or retrograde arterial perfusion during cardiopulmonary bypass. Intra-aortic balloon counter-pulsation use may also trigger aortic dissection. There is increased risk of type A TAD after aortic valve replacement, especially with larger aortic diameters.14 Finally, diagnostic angiography and cardiac catheterization may be complicated by aortic dissection (see Table 33.1).14 Table 33.1 Specific Risk Factors for Thoracic Aortic Dissection *Cocaine, amphetamine, sildenafil. †Bi-aortic value, aortic coarctation. ‡Marfan syndrome, Ehlers-Danlos syndrome, Turner syndrome, familial TAD. The aortic wall is composed of three layers: the innermost intima, the media (smooth muscle and elastic connective tissue), and the outermost adventitia. Hemodynamic stresses to the aortic inner walls can result from risk factors such as prolonged hypertension or inherently weakened connective tissue walls as seen in some connective tissue syndromes or a bicuspid aortic valve that alters the flow pattern of blood ejected out of the aorta. A dissection may be initiated by a tear or ulceration of the medial layer facilitated by degeneration from normal aging or compounded by the risk factors listed in Table 33.1. A classic aortic dissection is classified by an intimal tear into the media of the aortic wall, resulting in separation of the medial layer and formation of a false channel, allowing blood to flow into this channel. An intramural hematoma (IMH) can also be the trigger for a dissection when an accumulation of blood separates the medial layers; in this circumstance, the inciting entrance tear is lacking. IMH is more common in the elderly hypertensive patient’s descending aorta. Finally, aortic ulcers can disrupt the aortic wall and result in aortic rupture or dissection. Patients with aortic ulcers are older than those with IMH. The false lumen of a TAD has the potential to extend both distally and proximally, potentially leading to obstruction of arterial origins from the aortic trunk, rupture back into the true vascular lumen (which can be lifesaving), extension into the pericardial sac with pericardial tamponade, or rupture into the pleural cavity with devastating hemorrhagic shock and death (Fig. 33.2A,B). Rupture is the most common cause of death during the early acute phase of TAD. The most frequent rupture route leading to death is into the pericardium causing tamponade. Compromise of arch vessels may lead to neurologic symptoms and injury. Death may also occur with involvement of the aortic root, producing primary ostial compromise and acute myocardial infarction or severe aortic regurgitation. Rarely, fistulas and high-degree heart block may be produced. The thin wall of any residual pseudo-aneurysm following TAD tends to enlarge and over time is at high risk of rupture. Total thrombosis of the false lumen is rare, whereas distal reentry into the true lumen may help decompress the false lumen and increase the chance of survival. Postoperative false lumen patency is a predictor of late mortality.15 The diagnosis of acute TAD is complicated by the infrequent occurrence of this clinical condition as well as the diagnostic difficulty and is particularly problematic because of the potential catastrophic outcome.16 Typical symptoms of TAD are excruciating, severe at onset, pain of a sharp and tearing nature. The location of the pain (anterior chest, neck, jaw, inner scapular, and lumbar/abdominal) is linked to the location of the dissection. Symptoms, other than pain, include visceral symptoms (vomiting, diaphoresis, and syncope). Although physical examination findings may be absent, if present, they are useful in directing the clinician’s attention to this diagnosis.16 Inequality of pulses in the upper extremity and a blood pressure differential of 20 to 30 mm Hg between the two extremities may be seen based on the location of the dissection. A new aortic regurgitation murmur occurs in a significant number of patients. Proximal dissection may also interfere with coronary artery blood flow, producing cardiogenic shock or rupture into the pericardium, producing pericardial tamponade. Pericardial tamponade would be supported by findings of jugular venous distention, muffled heart tones, tachycardia, and hypotension. Mass compression effects can produce findings such as superior vena cava syndrome, Horner syndrome, hoarseness, dyspnea, or dysphagia. Syncope is seen in 1 of 10 cases of TAD. Syncope likely results from acute cardiac dysfunction or vascular outflow obstruction of the carotid arteries. Vasovagal pain response may also be a potential etiology of syncope. When syncope is related to hypovolemic shock from rupture through the adventitia into the pleural space, the prognosis is grave. The great majority of patients with thoracic aortic dissection has abnormalities on the chest radiograph. A normal chest radiograph may therefore help in decreasing the likelihood of aortic dissection. A study by Klompas looked at 1337 chest radiographs in patients with thoracic aortic dissection and reported abnormalities in 90% of patients.17 The most common changes associated with dissection are abnormal aortic contour, widening of the mediastinum, pleural effusion, displacement of intimal calcification, abnormalities of the aortic knob, and displacement of the trachea or nasogastric tube to the right. In the absence of an abnormal aortic contour or mediastinal widening, a diagnosis of dissection is less likely. The most common diagnostic modality used for diagnosis of TAD is computed tomography (CT) (Fig. 33.3). A CT angiogram shows high sensitivity and specificity in diagnosis and exclusion of TAD. It is the optimal imaging modality for ruling out aortic dissection in patients with low clinical pretest probability. Limitations of this technique include use of ionizing radiation and contrast media, need for transfer to imaging station, and limited ability to access the aortic valve. Advantages are ready availability, turnaround time, delineation of entire aorta, and diagnosis of other disorders causing the patient’s symptoms. Advances in CT angiographic techniques—such as spiral multidetection scanner technology that allows volume-rendered, three-dimensional reconstruction of a CT angiogram—are likely superior to magnetic resonance images (see Fig. 33.4 as an example of the technology). Transthoracic echocardiography (TTE) should be performed early in the evaluation of any patient in whom the diagnosis of ascending aortic dissection is entertained. If a pericardial effusion is present, signs of tamponade can be identified. TTE can help identify aortic dissection if multiple views are obtained—specifically, suprasternal, subcostal, and right parasternal views. The intimal flap may be identified within the lumen, with motion that is not synchronized with the surrounding structures. To minimize the chance of a false-positive result, the flap should be visualized in more than one view. The addition of color Doppler helps to identify flow artifacts (as opposed to an intimal flap) within the ascending aorta by demonstrating flow between the true and false channels at the site of an intimal tear and by showing a difference in the timing or direction of flow within the two lumens.18 Color Doppler permits detection and quantification of aortic regurgitation. TTE is especially useful for diagnosing dissections involving the ascending aorta but is much less sensitive for descending dissections. If a dissection is not visualized in the patient with chest pain, finding regional wall motion abnormalities may suggest the alternative diagnosis of coronary ischemia. Transthoracic echocardiography (TEE) (Fig. 33.5) can be performed safely on most critically ill patients in a monitored setting.19,20 To avoid precipitating hypertension, tachycardia, or gagging (straining) in a patient with suspected dissection, conscious sedation should be administered. Nearly all of the thoracic aorta can be visualized, including most of the arch. The area from the distal ascending aorta to the midarch, however, is difficult to evaluate with TEE because of interposition of the airway between the esophagus and the aorta.21 The sensitivity of TEE for thoracic aortic dissection is close to 100%, but specificity is lower, owing primarily to reverberation artifacts that may be visualized within the ascending aorta, simulating an intimal flap.22 Color flow Doppler with TEE may demonstrate flow through or on either side of the suspected intimal flap (Fig. 33.6
Acute Aortic Dissection
Introduction
History
Types of TAD
Risk Factors for Thoracic Aortic Dissection
Age and gender
Smoking
Trauma
Atherosclerosis
Aortitis
Pregnancy
Hypertension
Diabetes mellitus
Drug use*
Congenital cardiovascular defects†
Connective tissue syndromes‡
Aortic dilatation
Pathophysiology
Diagnosis
Symptoms
Physical Exam
Imaging
Chest Radiograph
Computed Tomography
Echocardiography

Full access? Get Clinical Tree


Acute Aortic Dissection