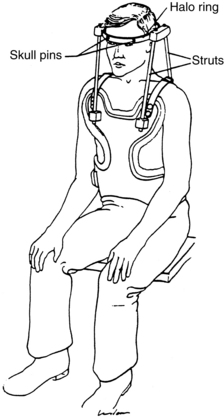
PROCEDURE 98 A halo ring attached to a halo vest (commonly referred to as a halo) is designed to immobilize and stabilize the cervical spine. A halo ring and vest may be used alone or in conjunction with surgery for the patient with an unstable cervical spine, as a result of spinal fracture or dislocation; degenerative processes, such as C1-C2 changes from rheumatoid arthritis; or spinal surgery. With the use of the halo ring and vest, vertebral column movement is prevented and subsequent risk of the injury to the spinal cord is reduced.2 The halo ring and vest may be used as a primary definitive treatment to stabilize the cervical spine, before surgery to reduce spine deformity, or after surgery as an adjunct to interval cervical fixation. This procedure focuses on the management of the patient who needs immobilization with a halo ring and vest. • Knowledge of neuroanatomy and physiology is necessary. • The nurse needs to be knowledgeable about the anatomy and physiology of the spinal column, the special anatomy of the cervical vertebrae, the spinal cord, and the cervical spinal nerves and their areas of peripheral innervation. In addition, the nurse must understand the pathophysiology and manifestations of spinal cord trauma, including spinal shock, ascending edema, and related impairment of respiratory function, vasomotor tone, and autonomic nervous system function. • The nurse must be knowledgeable about the signs and symptoms of new injury or extension of spinal cord injury and the needed interventions. • Immobilization assists in maintenance of vertebral alignment. In the case of an unstable vertebral column, it also reduces the risk for new injury to the spinal cord. • A number of treatment options are available to manage cervical injuries. The specific treatment for a particular patient depends on the type of injury, the level of injury (e.g., C2 as compared with C6), the specific classification of the injury, and patient characteristics. • A halo ring device is a graphite ring attached to the skull with four stabilizing pins (two anterior and two posterolateral; see Fig. 97-3). The pins are threaded through holes in the ring, screwed into the outer table of the skull, and locked into place. • Direct traction may be applied to the halo ring device with a rope and pulley or cable and bracket alignment system and weights (see Procedures 97 and 100). Patients with a halo ring, pins, and traction applied with weights are cared for similarly to patients in cervical traction with tongs (see Procedures 97 and 100). • When alignment of the cervical spine is achieved, long-term immobilization of the spine can be achieved by attaching the ring to a body vest or a custom molded body jacket, which allows for mobility of the patient (Fig. 98-1).2,3 • With the halo ring and pins in place, traction can be discontinued and a halo vest and struts added for long-term immobilization of the cervical neck (see Fig. 98-1). The advantage of this approach is that the patient can sit upright, mobilize out of bed, and ambulate, if able, while the cervical spine remains stable. • The nurse must be familiar with the components of the halo-vest device, including the halo ring and pins, anterior and posterior posts, vest screws, front and back panels of the vest, and shoulder and side buckles. • Basic cardiac life support knowledge and skills are essential. • It is important that the nurse knows how to access the patient’s anterior chest to administer cardiopulmonary resuscitation (CPR) if cardiac arrest occurs. Refer to information from the manufacturer of the halo vest for specific information on emergency access to the chest. Some vests have a hinged closure; the vest can be lifted up at the hinge to allow quick access to the chest. Other vests are not hinged and require a wrench. The wrench must be available at all times and, depending on institution policy, may be maintained on the front of the vest for instant access to the chest. If the patient needs defibrillation, avoid touching the bars of the traction with the defibrillator. • The halo-vest side panels may be opened only when the patient is flat and supine.2,5,8 Unbuckling of the halo vest may result in loss of spine alignment and neurologic compromise.8 Follow manufacturer’s recommendations and institution policies for opening the vest. • Because the halo vest limits movement of the head, patients must be taught to scan the environment for objects in their path that could lead to falls. • The halo vest changes the center of gravity and limits movement, thus requiring adaptations for performing activities of daily living (ADLs).8 • Soap and a basin of warm water
Halo Ring and Vest Care
PREREQUISITE NURSING KNOWLEDGE
EQUIPMENT
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 20: Chest Tube Placement (Perform)
20: Chest Tube Placement (Perform)
![]() 95: Lumbar Puncture (Perform)
95: Lumbar Puncture (Perform)
![]() 35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes
35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes

Full access? Get Clinical Tree


98: Halo Ring and Vest Care