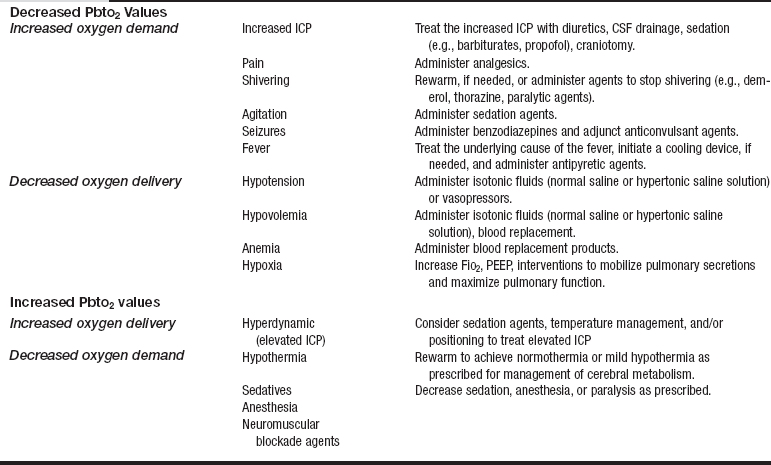
PROCEDURE 87 • Incorporated as an adjunct monitor of trends in concert with concurrent neurologic multimodality monitoring parameters (intracranial pressure [ICP], cerebral perfusion pressure [CPP], systemic jugular venous oxygen [SjVO2]), brain tissue oxygen saturation (also abbreviated as PbtO2, PbrO2, PtiO2, tiO2) monitoring reflects the oxygenation of cerebral tissue local to the sensor placement.4,22,30 • In institutions where SjVO2 is used as a monitoring parameter, the difference between SjVO2 measurements and PbtO2 values must be noted. SjVO2 is a measure of the oxygen contained in the blood draining from the cerebral venous sinuses into the jugular bulb (a measure of global brain oxygenation), whereas PbtO2 measures regional (local to the catheter placement in the cerebral white matter) brain tissue oxygenation.22,24,26 • Understanding of neuroanatomy and physiology, specifically intracranial dynamics, is needed. • Knowledge of sterile and aseptic technique is necessary. • Currently, only one brain tissue oxygen monitoring system is available.24 • A brain tissue oxygen probe may be inserted through an intracranial bolt or tunneled.2,30 • PbtO2 monitoring provides information that reflects brain tissue oxygen levels associated with cerebral oxygen demand and systemic oxygen delivery. • PbtO2 values are relative within an individual. Establishing and following the patient’s cerebral oxygen trends provides the healthcare providers with information that will aid in the assessment and treatment of cerebral hypoxia. • Indications for PbtO2 monitoring include patients at risk for secondary injury from cerebral edema. Conditions most likely to cause cerebral edema include severe traumatic brain injury, aneurysmal and traumatic subarachnoid hemorrhage, brain tumor, stroke, and any condition that increases ICP. • Contraindications for PbtO2 monitoring include patients with a coagulopathy, those receiving anticoagulation therapy, and those with an insertion site infection. • PbtO2 probes are safe with a 1.5-T magnetic resonance imaging (MRI) system as long as the fiberoptic ICP catheter is not in place.11 • PbtO2 probes are safe with computed tomography (CT). • Cerebral oxygen data are accurate and reliable when the PbtO2 probe is located in the deep white matter of the brain, the location where oxygen availability is most stable. • Parameters such as ICP and brain tissue temperature can be measured immediately at the time of probe placement. • Monitoring of PbtO2 values may be delayed as long as 2 hours as time is needed for the brain tissue to settle after the microtrauma caused by probe placement.5–7,12,28 • The normal range for brain tissue oxygen values is between 20 and 35 mm Hg.12,13,17,18,24 Treatment goals usually aim to keep the PbtO2 equal to or greater than 20 mm Hg.30 • A PbtO2 of less than 15 mm Hg is a critical threshold associated with a greater chance of functional disability and mortality related to cerebral ischemia.1,3,12,25 • A PbtO2 of less than 10 mm Hg is directly associated with severe disability, poor outcome at discharge, and death.1,3,28 • A PbtO2 of less than 5 mm Hg is indicative of cerebral cell death and an approximately 90% mortality rate.1,3,14,23,25 • Brain tissue oxygen values can be used to manage potential cerebral hypoxia. Clinical interventions can be aimed at increasing oxygen delivery or decreasing cerebral oxygen demand. • Decreases in PbtO2 values occur when cerebral blood flow or cerebral oxygen delivery is inadequate or states of increased metabolic demands exist, indicating the potential for secondary brain injury. • Increases in PbtO2 values denote decreased oxygen uptake by cerebral cells that may be caused by states of increased oxygen delivery or decreased oxygen utilization. • Table 87-1 outlines treatment options for patients with a decrease or increase in PbtO2 values. • PbtO2 probe placement: The physician placing the probe device determines the catheter placement location after review of the CT scan and after consideration of the most appropriate monitoring area based on diagnosis and pathology, avoiding areas of infarct or hematoma.4,17 Placement of the probe may be ipsilateral or contralateral to the pathology.26
Brain Tissue Oxygen Monitoring: Insertion (Assist), Care, and Troubleshooting
PREREQUISITE NURSING KNOWLEDGE
 The probe may be placed in the nondominant hemisphere (e.g., right frontal region) to minimize risk of injury from catheter insertion.6,12,29 The right hemisphere is a safer location for probe placement than the left hemisphere because speech function is located in the left hemisphere in most individuals.
The probe may be placed in the nondominant hemisphere (e.g., right frontal region) to minimize risk of injury from catheter insertion.6,12,29 The right hemisphere is a safer location for probe placement than the left hemisphere because speech function is located in the left hemisphere in most individuals.
Related posts:
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]() 44: Emergent Open Sternotomy (Assist)
44: Emergent Open Sternotomy (Assist)

Full access? Get Clinical Tree


87: Brain Tissue Oxygen Monitoring: Insertion (Assist), Care, and Troubleshooting