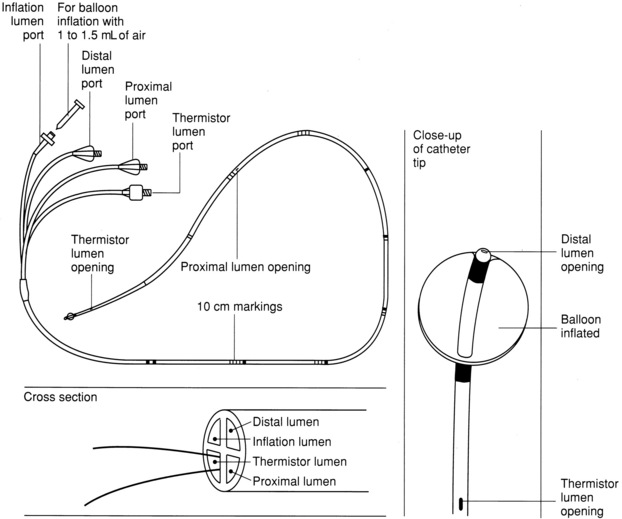
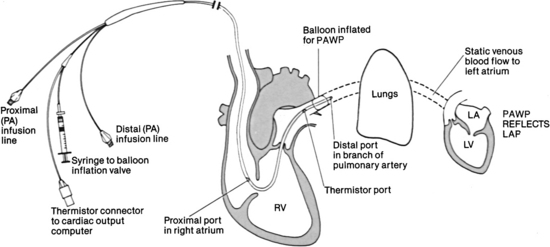
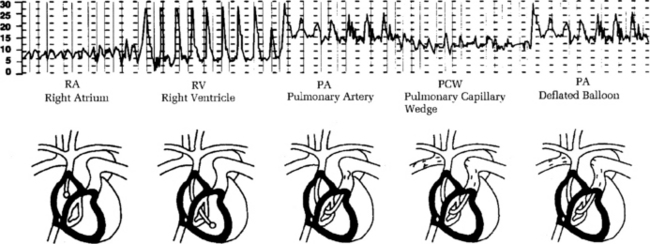
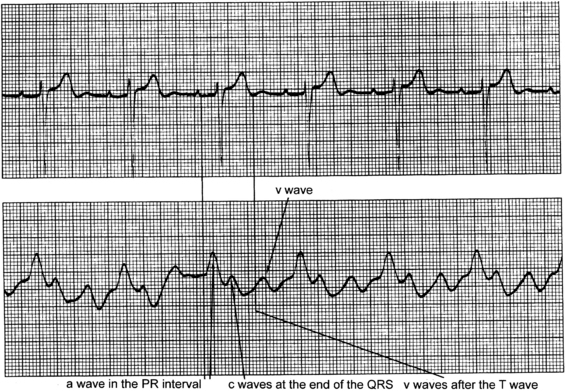
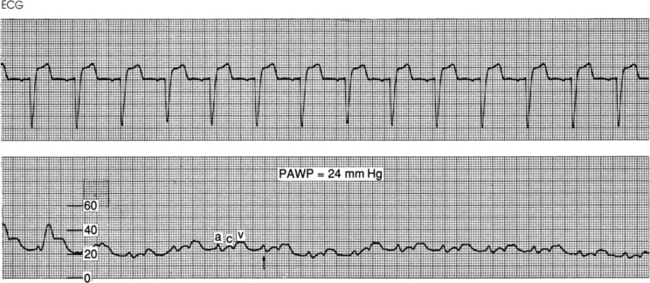
PROCEDURE 73 • Knowledge of the normal cardiovascular anatomy and physiology is needed. • Knowledge of the normal pulmonary anatomy and physiology is necessary. • Knowledge of principles of aseptic technique is needed. • Basic dysrhythmia recognition and treatment of life-threatening dysrhythmias should be understood. • Advanced cardiac life support knowledge and skills are necessary • Knowledge of the anatomy of the pulmonary artery (PA) catheter (Fig. 73-1) and the location of the PA catheter in the heart and pulmonary artery (Fig. 73-2) is important. • Knowledge of the setup of the hemodynamic monitoring system (see Procedure 76) is essential. • Understanding of normal hemodynamic values (see Table 67-1) is needed. • The pulmonary artery catheter contains a proximal injectate lumen port, a PA distal lumen port, a thermistor connector, and a balloon-inflation valve. Some catheters also have two infusion ports, right atrial (RA) and right ventricular (RV) lumens, that can be used for infusion of medications and intravenous fluids. • The PA distal lumen is used to monitor systolic, diastolic, and mean pressures in the pulmonary artery. This lumen also allows for sampling of mixed venous blood. The proximal injectate lumen is used to monitor the right atrial pressure and inject the solution used to obtain cardiac output (CO). The balloon-inflation valve is used to obtain the pulmonary artery occlusion pressure (PAOP). • PAOP may be referred to as pulmonary artery wedge pressure. • The PA diastolic pressure and the PAOP are indirect measures of left ventricular end-diastolic pressure (LVEDP). Usually, the PAOP is approximately 1 to 4 mm Hg less than the pulmonary artery diastolic pressure (PADP). Because these two pressures are similar, the PADP is commonly followed, which minimizes the frequency of balloon inflation, thus decreasing the potential of balloon rupture and pulmonary artery trauma. • Differences between the PADP and the PAOP may exist for patients with pulmonary hypertension, chronic obstructive lung disease, acute respiratory distress syndrome (ARDS), pulmonary embolus, and tachycardia. • Indications for PA catheter therapy (see Procedure 72 for additional indications) are as follows: • Hemodynamic monitoring with a PA catheter has no absolute contraindications, but an assessment of risk versus benefit to the patient should be considered. Relative contraindications to pulmonary artery catheter insertion include presence of fever, presence of a mechanical tricuspid valve, and a coagulopathic state. A patient with left bundle-branch block may have a right bundle-branch block develop during PA catheter insertion, resulting in complete heart block. In these patients, a temporary pacemaker should be readily available. • Pulmonary artery pressures may be elevated as a result of pulmonary artery hypertension, pulmonary disease, mitral valve disease, left ventricular failure, atrial or ventricular left-to-right shunt, pulmonary emboli, or hypervolemia. • Pulmonary artery pressures may be decreased due to hypovolemia or vasodilation. • Waveforms that occur during insertion include RA, RV, PA, and pulmonary artery occlusion (PAO; Fig. 73-3). Figure 73-4 Identification of a, c, and v waves in the waveform for right atrial and central venous pressure (RA/CVP). Atrial waveforms are characterized by three components: a, c, and v waves. The a wave reflects atrial contraction, the c wave reflects closure of the tricuspid valve, and the v wave reflects passive filling of the atria. (From Ahrens TS, Taylor LK: Hemodynamic waveform analysis, Philadelphia, 1992, Saunders.) Figure 73-5 Normal pulmonary artery occlusion pressure (PAOP) waveform. Note the delay in the a, c, and v waves because of the time needed for the mechanical events to show a pressure change. This waveform is from a spontaneously breathing patient. The arrow indicates end expiration, where the mean of a wave pressure is measured. Pulmonary artery occlusion pressure (PAOP) is also referred to as pulmonary artery wedge pressure (PAWP). • Insertion and placement verification should occur as follows: • PA catheter (non–heparin-coated PA catheters and latex-free PA catheters are available) • Percutaneous sheath introducer kit and sterile catheter sleeve • Pressure modules and cables for interface with the monitor
Pulmonary Artery Catheter Insertion (Assist) and Pressure Monitoring
PREREQUISITE NURSING KNOWLEDGE
 Aid in the diagnosis of complications after acute myocardial infarction (MI), which may include heart failure, cardiogenic shock, papillary muscle rupture, mitral regurgitation, ventricular septal rupture, or cardiac rupture with tamponade.
Aid in the diagnosis of complications after acute myocardial infarction (MI), which may include heart failure, cardiogenic shock, papillary muscle rupture, mitral regurgitation, ventricular septal rupture, or cardiac rupture with tamponade.
 Assessment of ventricular function in heart failure.
Assessment of ventricular function in heart failure.
 The a wave reflects atrial contraction, the c wave reflects closure of the atrioventricular valve, and the v wave reflects passive filling of the atria during ventricular systole (Figs. 73-4 and 73-5).
The a wave reflects atrial contraction, the c wave reflects closure of the atrioventricular valve, and the v wave reflects passive filling of the atria during ventricular systole (Figs. 73-4 and 73-5).
 Elevated v waves in the RAP/CVP waveform may occur in patients with tricuspid insufficiency.
Elevated v waves in the RAP/CVP waveform may occur in patients with tricuspid insufficiency.
 The PA catheter may be inserted through the subclavian, internal jugular, femoral, external jugular, or antecubital veins.
The PA catheter may be inserted through the subclavian, internal jugular, femoral, external jugular, or antecubital veins.
 The standard 7.5 Fr PA catheter is 110 cm long and has black markings at 10-cm increments and wide black markings at 50-cm increments for facilitation of insertion and positioning (see Fig. 73-1). The catheter should reach the PA after being advanced 40 to 55 cm from the internal jugular vein, 35 to 50 cm from the subclavian vein, 60 cm from the femoral vein, 70 cm from the right antecubital fossa, and 80 cm from the left antecubital fossa.
The standard 7.5 Fr PA catheter is 110 cm long and has black markings at 10-cm increments and wide black markings at 50-cm increments for facilitation of insertion and positioning (see Fig. 73-1). The catheter should reach the PA after being advanced 40 to 55 cm from the internal jugular vein, 35 to 50 cm from the subclavian vein, 60 cm from the femoral vein, 70 cm from the right antecubital fossa, and 80 cm from the left antecubital fossa.
 Catheter placement is also verified with chest radiography.
Catheter placement is also verified with chest radiography.
EQUIPMENT
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter

Full access? Get Clinical Tree


73: Pulmonary Artery Catheter Insertion (Assist) and Pressure Monitoring