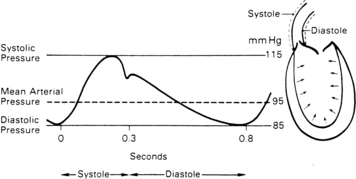
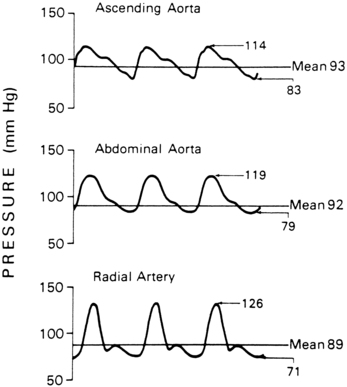
PROCEDURE 62 • Knowledge of the anatomy and physiology of the vasculature and adjacent structures is needed. • Knowledge of the principles of hemodynamic monitoring is necessary. • Understanding of the principles of aseptic technique is needed. • Conditions that warrant the use of arterial pressure monitoring include patients with: • Arterial pressure represents the forcible ejection of blood from the left ventricle into the aorta and out into the arterial system. During ventricular systole, blood is ejected into the aorta, generating a pressure wave. Because of the intermittent pumping action of the heart, this arterial pressure wave is generated in a pulsatile manner (Fig. 62-1). The ascending limb of the aortic pressure wave (anacrotic limb) represents an increase in pressure because of left ventricular ejection. The peak of this ejection is the peak systolic pressure, which should be less than 120 mm Hg in adults.18 After reaching this peak, the ventricular pressure declines to a level below aortic pressure and the aortic valve closes, marking the end of ventricular systole. The closure of the aortic valve produces a small rebound wave that creates a notch known as the dicrotic notch. The descending limb of the curve (diastolic downslope) represents diastole and is characterized by a long declining pressure wave, during which the aortic wall recoils and propels blood into the arterial network. The diastolic pressure is measured as the lowest point of the diastolic downslope, which should be less than 80 mm Hg in adults.18 • The difference between the systolic and diastolic pressures is the pulse pressure, with a normal value of about 40 mm Hg. • Arterial pressure is determined by the relationship between blood flow through the vessels (cardiac output) and the resistance of the vessel walls (systemic vascular resistance). The arterial pressure is therefore affected by any factors that change either cardiac output or systemic vascular resistance. • The average arterial pressure during a cardiac cycle is called the mean arterial pressure (MAP). MAP is not the average of the systolic plus the diastolic pressures because during the cardiac cycle, the pressure remains closer to diastole than to systole for a longer period (at normal heart rates). The MAP is calculated automatically by most patient monitoring systems; however, it can be calculated with the following formula: • MAP represents the driving force (perfusion pressure) for blood flow through the cardiovascular system. MAP is at its highest point in the aorta. As blood travels through the circulatory system, systolic pressure increases and diastolic pressure decreases, with an overall decline in the MAP (Fig. 62-2). • The location of arterial catheter placement depends on the condition of the arterial vessels and the presence of other catheters (i.e., the presence of a dialysis shunt is a contraindication for placement of an arterial catheter in the same extremity). Once inserted, the arterial catheter causes little or no discomfort to the patient and allows continuous blood pressure assessment and intermittent blood sampling. If intraaortic balloon pump therapy is necessary, arterial pressure may be directly monitored from the tip of the balloon in the aorta. • The radial artery is the most common site for arterial pressure monitoring. When arterial pulse waveforms are recorded from a peripheral site (instead of a central site), the waveform morphology changes. The anacrotic limb becomes more peaked and narrowed, with increased amplitude; therefore, the systolic pressure in peripheral sites is higher than the systolic pressure recorded from a more central site (see Fig. 62-2). In addition, the diastolic pressure decreases, the diastolic downslope may show a secondary wave, and the dicrotic notch becomes less prominent from distal sites. • Vasodilators and vasoconstrictors may change the appearance of the waveforms from distal sites. Vasodilators may cause the waveform to take on a more central appearance. Vasoconstrictors may cause the systolic pressure to become more exaggerated because of enhanced resistance in the peripheral arteries. • Several potential complications are associated with arterial pressure monitoring. Infection at the insertion site can develop and cause sepsis. Clot formation in the catheter can lead to arterial embolization. The catheter can cause vessel perforation with extravasation of blood and flush solution into the surrounding tissue. Finally, the distal extremity can develop circulatory or neurovascular impairment. • 1- to 2-inch (2.5- to 5-cm) over-the-needle catheter (14-gauge to 20-gauge for adults) or prepackaged kit with catheter, introducer, and guidewire • Single-pressure transducer system (see Procedure 76) • Monitoring equipment consisting of a connecting cable, monitor, oscilloscope display screen, and recorder • Nonsterile gloves, head coverings, goggles • Antiseptic solution (e.g., 2% chlorhexidine-based preparation)
Arterial Catheter Insertion (Assist), Care, and Removal
PREREQUISITE NURSING KNOWLEDGE
 Hemodynamic instability (e.g., acute hypotension, hypertensive crisis)
Hemodynamic instability (e.g., acute hypotension, hypertensive crisis)
 Shock from any cause (e.g., hemorrhagic, septic)
Shock from any cause (e.g., hemorrhagic, septic)
 Continuous infusion of vasoactive medications
Continuous infusion of vasoactive medications
 Intraaortic balloon pump therapy
Intraaortic balloon pump therapy
 Coronary interventional procedures
Coronary interventional procedures
 Major surgical procedures (e.g., neurologic, abdominal, cardiac, thoracic, vascular, trauma)
Major surgical procedures (e.g., neurologic, abdominal, cardiac, thoracic, vascular, trauma)

EQUIPMENT
Related posts:
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]() 44: Emergent Open Sternotomy (Assist)
44: Emergent Open Sternotomy (Assist)

Full access? Get Clinical Tree


62: Arterial Catheter Insertion (Assist), Care, and Removal