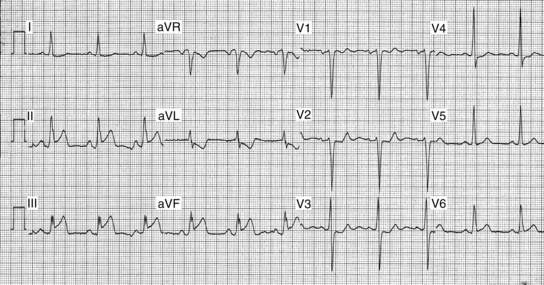
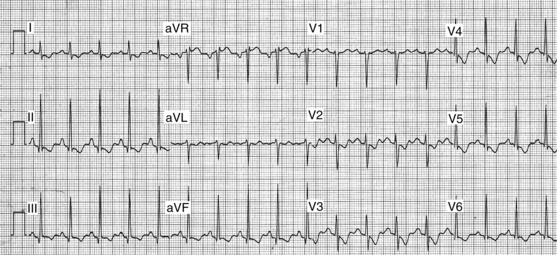
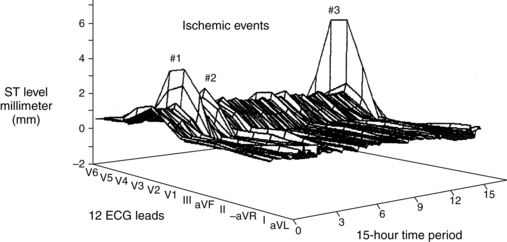
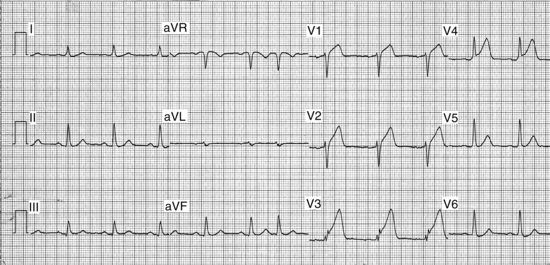
PROCEDURE 59 Bedside ST-segment monitoring provides ongoing surveillance for detection of transient myocardial ischemia. This technology should be applied to patients who are being evaluated or are diagnosed with acute coronary syndrome, including acute myocardial infarction and unstable angina.2,3,8,13,16 For these patients, continuous ST-segment monitoring is valuable in determining the success of thrombolytic therapy and percutaneous coronary intervention and detecting recurrent or transient ischemia. The goal of continuous ST-segment monitoring is to detect new or recurrent myocardial ischemia. • Understanding of the anatomy and physiology of the cardiovascular system, principles of cardiac conduction, electrocardiogram (ECG) lead placement, basic dysrhythmia interpretation, and electrical safety is needed. • Advanced cardiac life support knowledge and skills are necessary. • Continuous monitoring of the ECG for ischemic ST-segment changes is more reliable than patient symptoms because more than three quarters of ECG-detected ischemic events are clinically silent.2,8,13,16 Patients who have transient ischemia detected with continuous ST-segment monitoring are more likely to have unfavorable outcomes, including myocardial infarction (MI) and death, compared with patients without such events.2,3,8,10,11,13,16 • Because of the dynamic, unpredictable, and silent nature of myocardial ischemia, continuous monitoring of patients for ischemia is essential. Clinicians should monitor the trend of the ST segments over time and evaluate any ST-segment changes (elevation or depression) for possible myocardial ischemia (Fig. 59-1). Figure 59-1 The importance of assessing the trend of the ST segments over time. The three-dimensional image illustrates ST-segment deviation in millimeters (Y-axis) in all 12 ECG leads (X-axis) over a 15-hour period (Z-axis). Illustrated are three separate ischemic events, characterized by ST-segment elevation, in leads V3 to V5. (Adapted from Pelter MM, Adams MG, Drew BJ: Transient myocardial ischemia is an independent predictor of adverse in-hospital outcomes in patients with acute coronary syndromes treated in the telemetry unit, Heart Lung 32:71-78, 2003.) • Other nonischemic causes for a change in the ST-segment trend are movement of the skin electrodes, dysrhythmias, intermittent bundle-branch block pattern, body position changes, and ventricular paced rhythms.8,12 • The first type of ischemia seen in patients with acute coronary syndrome (ACS) is supply-related ischemia from coronary occlusion. Coronary occlusion is brought on by disruption of an atherosclerotic plaque followed by cycles of plaque rupture, platelet stimulation, coronary vasospasm, and thrombus formation.5,6,14,19 Because this type of ischemia threatens the entire thickness of the myocardium, immediate treatment to reestablish blood flow to the heart is essential. The typical ECG manifestation of total coronary occlusion is ST-segment elevation visible in the ECG leads that lie directly over the ischemic myocardial zone. Occlusion of the right coronary artery (RCA) typically produces ST-segment elevation in leads II, III, and augmented vector foot or aVF (Fig. 59-2). Occlusion of the left anterior descending (LAD) coronary artery typically produces ST-segment elevation in leads V2, V3, and V4 (Fig. 59-3). Diagnosis of total coronary occlusion of the left circumflex coronary artery (LCX) is more complex because placement of the standard ECG electrodes is on the anterior chest, opposite the wall that this coronary artery supplies. Occlusion of the LCX may produce ST-segment depression in leads V1, V2, or V3, which reflects the reciprocal, or mirror image, ST-segment elevation occurring in the posterior wall of the myocardium. Figure 59-3 The typical ST-segment pattern of supply-related ischemia in the anterior wall. The LAD artery is likely occluded, resulting in ST-segment elevation in leads V2 to V4. • A second type of ischemia for which patients with ACS or stable angina are at risk is demand-related ischemia. This type of ischemia may occur when the demand for oxygen (i.e., exercise, tachycardia, or stress) exceeds the flow capabilities of a coronary artery with a stable atherosclerotic plaque. The ST-segment pattern of demand-related ischemia is depression, often appearing in several ECG leads (Fig. 59-4). • Diagnosis of myocardial ischemia necessitates continuous monitoring of all 12 ECG leads because the mechanism of ischemia may vary (i.e., occlusion versus demand-related ischemia), resulting in distinctly different ST-segment patterns (e.g., elevation or depression). If only two ECG leads are available, however, the best two are leads III and V3.8 Patient-specific monitoring also may be done if a prior 12-lead ECG was obtained during acute ischemia (i.e., ST-segment elevation MI, percutaneous coronary intervention [PCI], or treadmill test). In this scenario, the ECG lead or leads showing maximal ST-segment deviation should be selected for continuous monitoring to detect recurrent ischemia. • According to current consensus statements,8,9 multilead ST-segment monitoring is indicated in most patients with the following diagnoses:
Continuous ST-Segment Monitoring
PREREQUISITE NURSING KNOWLEDGE
 Early phase of acute MI (ST elevation, non-ST elevation, “rule-out”)
Early phase of acute MI (ST elevation, non-ST elevation, “rule-out”)Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 20: Chest Tube Placement (Perform)
20: Chest Tube Placement (Perform)
![]() 95: Lumbar Puncture (Perform)
95: Lumbar Puncture (Perform)
![]() 35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes
35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes

Full access? Get Clinical Tree


59: Continuous ST-Segment Monitoring