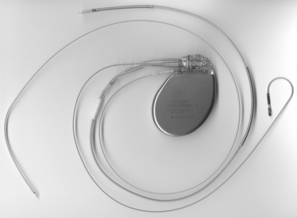
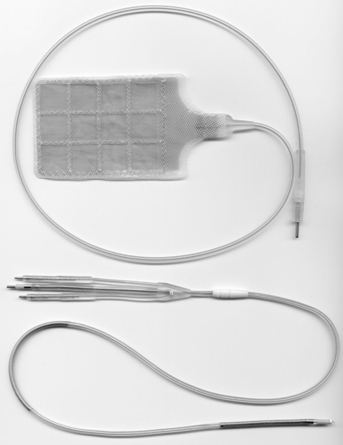
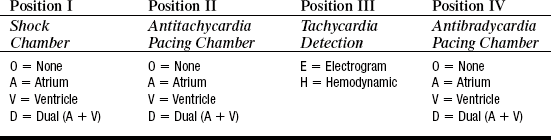
PROCEDURE 50 • Knowledge of the anatomy and physiology of the cardiovascular system, principles of cardiac conduction, and basic dysrhythmia interpretation is needed. • Knowledge of basic functioning of implantable cardioverter-defibrillators (ICDs) and patient response to ICD therapy is needed. • Knowledge of principles of defibrillation threshold, antidysrhthmia medications, alteration in electrolytes, and effect on the defibrillation threshold is necessary. • Advanced cardiac life support (ACLS) knowledge and skills are needed. • Clinical and technical competence related to use of the external defibrillator is necessary. • Indications for ICD implantation, based on the 2008 American College of Cardiology (ACC)/American Heart Association (AHA)/ Heart Rhythm Society (HRS) guidelines6: • The ICD system is composed of a pulse generator and a lead system. The pulse generator is titanium and contains the capacitors, circuitry, and a lithium battery (Fig. 50-1). • Battery longevity may be greater than 6 years, depending on the number of times therapies are delivered and the frequency of pacing.5 The pulse generator is typically located in a pectoral subcutaneous pocket. • The leads are insulated wires that sense the patient’s intrinsic rhythm and can pace or deliver therapies (Fig. 50-2). Leads are classified as atrial or ventricular, endocardial (transvenous) or epicardial (myocardial), unipolar or bipolar, and active or passive fixation.8 The lead systems may be single, double, or multiple. • Leads may be attached to the heart via active or passive fixation. Active fixation leads use a screw, barb, or hook at the tip that is embedded into the myocardium to ensure stability of the lead. Passive fixation leads use tines or fins at the tip that allow the lead to attach to trabeculae of the myocardium. • Most leads are endocardial (transvenous) leads and are inserted transvenously through the subclavian, cephalic, or axillary veins. • Epicardial leads are less common but are used in special circumstances. Epicardial pacing leads may be placed on the outside of the left ventricular to provide biventricular pacing when coronary sinus placement of the LV lead has been unsuccessful. Epicardial patches may be placed on the outside of the heart, both anteriorly and posterior. Epicardial patches provide a greater surface area for defibrillation (See Fig. 50-2). • All leads have a cathode (negative pole) and an anode (positive pole). A unipolar lead uses one conductor wire, with a distal electrode as cathode and the metal can as the anode. This configuration produces a large electrical circuit and a large pacing artifact on electrocardiography (ECG). Because of the large area covered, this configuration is susceptible to stimulation of chest muscles and also to electromagnetic interference. A bipolar lead uses two electrodes on the distal end of the lead to form the circuit. The cathode is located at the distal tip, and the anode several millimeters proximal to the tip. Because of the closer circuitry, a smaller pacing artifact is seen on ECG. • All ICDs function as pacemakers. Some ICDs are also biventricular pacemakers. Cardiac resynchronization therapy (CRT) paces the right and left ventricles together to establish synchrony in an effort to improve LV function. CRT is considered for patients with symptomatic heart failure, optimized medical therapy, LVEF less than 35%, and prolonged QRS duration of greater than 120 milliseconds.1 Biventricular pacing must be as close to 100% as possible for the greatest benefit. Biventricular pacing leads are placed in the right atrium, the right ventricle, and an epicardial vein on the surface of the left ventricle accessed through the coronary sinus. • The ICD detects tachydysrhythmias, delivers antitachycardia pacing (ATP) or electrical therapy (shock), and provides bradycardia pacing. ATP attempts to convert monomorphic VT by pacing at a rate faster than the VT rate, thereby terminating the dysrhythmia. ATP is a painless way of treating VT, sometimes avoiding shock therapy altogether. The PainFree II trial demonstrated that compared with shocks, empirical ATP for fast VT was highly effective, equally safe, and, improved quality of life.17 Cardioversion is generally referred to as synchronized electrical therapy. Defibrillation is not synchronized and is generally used to convert ventricular dysrhythmias. • The ICD therapies may be programmed from one to three zones. Typically, the zones are labeled as 1, VT, usually at slower VT rates of 140 to180 beats per minute (varies according to physician preference and patient situation); 2, fast VT, usually at rates in the range of 180 to 220 beats per minute or higher; and 3, VF for rates usually greater than 220 beats per minute. VT zones may be programmed for sequential therapies of ATP followed by electrical defibrillation if ATP is unsuccessful. • A defibrillator code was developed in 1993 by the North American Society of Pacing and Electrophysiology and the British Pacing and Electrophysiology Group to describe the capabilities and operation of ICDs. The defibrillator code is patterned after the pacemaker code; however, it has some important differences (Table 50-1).2 The defibrillator code offers less information about the ICD’s antibradycardia pacing function but more specific information about the shock functions. Table 50-1
Implantable Cardioverter-Defibrillator
PREREQUISITE NURSING KNOWLEDGE
 Survivors of cardiac arrest as a result of ventricular fibrillation (VF) or sustained unstable ventricular tachycardia (VT)
Survivors of cardiac arrest as a result of ventricular fibrillation (VF) or sustained unstable ventricular tachycardia (VT)
 Patients with structural heart disease and sustained VT
Patients with structural heart disease and sustained VT
 Patients with unexplained syncope, significant left ventricular (LV) dysfunction, nonischemic DCM
Patients with unexplained syncope, significant left ventricular (LV) dysfunction, nonischemic DCM
 Patients with sustained VT with normal or near-normal ventricular function
Patients with sustained VT with normal or near-normal ventricular function
 Patients with long QT syndrome who are having syncope or VT while receiving beta blockers
Patients with long QT syndrome who are having syncope or VT while receiving beta blockers
 Patients who are not hospitalized and await transplantation
Patients who are not hospitalized and await transplantation
 Patients with cardiac sarcoidosis, giant cell myocarditis, or Chagas’ disease
Patients with cardiac sarcoidosis, giant cell myocarditis, or Chagas’ disease
 Class IIb: May be considered in:
Class IIb: May be considered in:
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 20: Chest Tube Placement (Perform)
20: Chest Tube Placement (Perform)
![]() 95: Lumbar Puncture (Perform)
95: Lumbar Puncture (Perform)
![]() 35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes
35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes

Full access? Get Clinical Tree


50: Implantable Cardioverter-Defibrillator