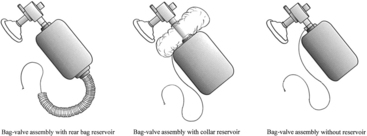
PROCEDURE 32 • Bagging is an essential skill used in emergency situations, such as cardiopulmonary arrest. Bagging also is indicated for the following: • Manual self-inflating resuscitation bag-valve device (of appropriate size) (Fig. 32-2) and appropriately sized mask • Oxygen source, flow regulator, and tubing • PEEP valve or PEEP attachment (if patient on greater than 10 cm H2O of PEEP) • Personal protective equipment (i.e., gloves, mask, goggles, gown, as appropriate) Additional equipment to have available depending on patient need: • Oxygen analyzer when specific fraction (i.e., lower than 100%) of inspired oxygen (FiO2) is desired
Manual Self-Inflating Resuscitation Bag-Valve Device
PREREQUISITE NURSING KNOWLEDGE
 To provide oxygenation and ventilation before and after suctioning airway procedures and during patient transports
To provide oxygenation and ventilation before and after suctioning airway procedures and during patient transports
 To assess airway patency and proper airway device placement
To assess airway patency and proper airway device placement
 To evaluate the interaction of patient and ventilator
To evaluate the interaction of patient and ventilator
 To alter the ventilatory pattern
To alter the ventilatory pattern
 Bagging should result in chest movement and auscultatory evidence of bilateral air entry.
Bagging should result in chest movement and auscultatory evidence of bilateral air entry.
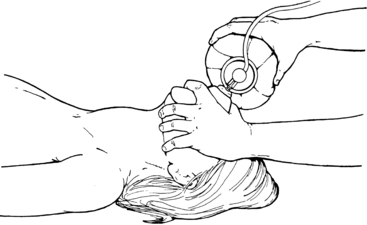
 In patients without an artificial airway in place, effective bagging requires an unobstructed airway, slight head and neck hyperextension (i.e., the same technique used for mouth-to-mouth ventilation), and firm placement of the face mask over the nose and mouth (Fig. 32-1). An exception to this technique is with known or suspected cervical spine injury, in which the patient’s airway is opened with the chin-lift method (without neck hyperextension). Effective bagging is best accomplished with two people: one to secure the mask and ensure head and neck placement and one to bag.1 In patients with artificial airways, such as endotracheal or nasotracheal tubes or tracheostomies, the nurse must understand the components of artificial airways and their relationship to the upper airway anatomy (see Procedures 1, 2, 3, 7, 8, 9, 12, 13, 14, 18).
In patients without an artificial airway in place, effective bagging requires an unobstructed airway, slight head and neck hyperextension (i.e., the same technique used for mouth-to-mouth ventilation), and firm placement of the face mask over the nose and mouth (Fig. 32-1). An exception to this technique is with known or suspected cervical spine injury, in which the patient’s airway is opened with the chin-lift method (without neck hyperextension). Effective bagging is best accomplished with two people: one to secure the mask and ensure head and neck placement and one to bag.1 In patients with artificial airways, such as endotracheal or nasotracheal tubes or tracheostomies, the nurse must understand the components of artificial airways and their relationship to the upper airway anatomy (see Procedures 1, 2, 3, 7, 8, 9, 12, 13, 14, 18).
 When signs and symptoms of respiratory distress are noted in a patient on mechanical ventilation, the patient should be bagged on 100% oxygen if troubleshooting the ventilator does not immediately solve the problem. Large bagged breaths or rapid rates during bagging may result in dynamic hyperinflation and resultant hypotension.2,3 Hyperinflation occurs when exhalation time is inadequate, which results in auto–positive end-expiratory pressure (auto-PEEP) and decreased venous return (see Procedure 30), with the resultant hypotension. Dynamic hyperinflation is most commonly associated with bronchospasm and chronic obstructive pulmonary disease.2 A high index of suspicion for the presence of dynamic hyperinflation is necessary if hypotension occurs with bagging. A brief disconnection from the bag or the provision of longer exhalation times or both results in a rapid increase in blood pressure. Bagging is resumed at a slower rate and with longer expiratory times.
When signs and symptoms of respiratory distress are noted in a patient on mechanical ventilation, the patient should be bagged on 100% oxygen if troubleshooting the ventilator does not immediately solve the problem. Large bagged breaths or rapid rates during bagging may result in dynamic hyperinflation and resultant hypotension.2,3 Hyperinflation occurs when exhalation time is inadequate, which results in auto–positive end-expiratory pressure (auto-PEEP) and decreased venous return (see Procedure 30), with the resultant hypotension. Dynamic hyperinflation is most commonly associated with bronchospasm and chronic obstructive pulmonary disease.2 A high index of suspicion for the presence of dynamic hyperinflation is necessary if hypotension occurs with bagging. A brief disconnection from the bag or the provision of longer exhalation times or both results in a rapid increase in blood pressure. Bagging is resumed at a slower rate and with longer expiratory times.
EQUIPMENT
Related posts:
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]() 44: Emergent Open Sternotomy (Assist)
44: Emergent Open Sternotomy (Assist)

Full access? Get Clinical Tree


32: Manual Self-Inflating Resuscitation Bag-Valve Device