CHAPTER 25. Abdominal Emergencies
Reneé Semonin Holleran
Competencies



1. Perform a comprehensive assessment of the patient with an abdominal emergency.
2. Initiate the critical interventions for the management of an abdominal emergency during transport.
3. Identify the management of specific abdominal emergencies during transport.
Disorders encountered by transport teams may include esophageal obstruction and esophageal varices with rupture; stomach disorders, such as gastric or duodenal hemorrhage, ulceration, perforation, or pyloric obstruction; gallbladder and biliary tract disorders; liver disease; pancreatic disorders; and intestinal obstruction or rupture, ruptured diverticula, and acute appendicitis.
Transport via air may cause specific problems for the patient with an abdominal emergency. 11 The aerodynamics and biophysics that govern air medical care are especially important in relation to the gastrointestinal (GI) system, which encompasses 26 ft of liquid-producing and gas-producing viscous matter. Careful patient history, assessment, and pretransport planning are imperative for the patient transported via air. 1
ESOPHAGUS
The esophagus is a hollow tube of striated and smooth muscle that is approximately 10 inches long in an adult. It lies posteriorly to the trachea, closely aligns the left mainstem bronchus, and exits the thoracic cavity at the diaphragmatic hiatus, or approximately at the T11 level. The esophagus provides the primary functions of peristaltic movement of food bolus, prevention of reflux with lower esophageal sphincter activity, and venting for gastric pressure changes.
Vascular supply to the esophagus is through branches of the descending thoracic aorta. Venous return from the esophagus is through the superior vena cava, azygos system, and portal vein system.
Neurologic intervention is initiated in the medulla and carried out by the vagus nerve. Because the esophagus lies in the thoracic cavity, in normal atmospheric conditions, it maintains a subatmospheric pressure of –5 to –10 mm Hg, whereas the stomach, which is in the abdominal cavity, rests at an atmospheric pressure of +5 to +10 mm Hg. Acute esophageal occurrences are esophageal obstruction, esophageal varices, and esophageal rupture.
Esophageal Obstruction
Three areas in the esophagus are narrow and may be potential sites for obstruction and injury. These areas include the cricoid cartilage, the arch of aorta, and the point at which the esophagus passes through the diaphragm. 6
Esophageal obstruction is fairly common. Strictures, webs, tumors, diverticula, foreign bodies, achalasia, and lower esophageal rings can all reduce or eliminate the venting property of the esophagus for the upper GI system. When air medical transport of a patient with obstruction is undertaken, intermittent exposure to variations in altitude is of great importance. Esophageal obstruction and an expanding gastrum can pose a serious threat if rapid decompression occurs at 35,000 ft. The venting property needs to be established before flight and depends on whether rotor-wing or fixed-wing transport is to be used. 11
Assessment
The transport team should correlate careful physical assessment with interpretation of radiologic and laboratory data to anticipate any potential problems that may occur during the transport process.
Subjective Data
The transport team should ascertain the patient’s chief symptom and medical history. Included in these subjective data should be the patient’s clinical course since the incident occurred. Medical history helps the transport team identify any other additional problems that may arise during transport.
Objective Data
The flight nurse performs a physical examination that includes assessment of the following:
▪ The patient’s ability to protect the airway.
▪ The patient’s ability to clear secretions by swallowing.
▪ The presence and location of pain.
Diagnostic Tests
Radiographic studies of the obstruction should accompany the patient. If an esophagoscopy has been performed, a report should be provided to the transport team so they can prepare for any potential problems that may occur during transport.
Plan and Implementation
If the patient is being transported via air, the plan of care depends on the anticipated transport altitude. The transport team should carefully evaluate the patient’s ability to maintain the airway. Even with aircraft pressurization, adequate gastric venting is extremely important if high altitude will be maintained. Pretransport medications and antiemetic therapy are often helpful not only for the antiemetic effect but also for the associated drowsiness. A gastric tube should be placed (if not contraindicated) and gastric contents emptied before and during transport. If the gastric tube is hooked to suction, its flow and contents should be closely monitored during transport. Continuous monitoring of respiratory status is also necessary.
Intervention
Caution must be exercised when a patient is placed on suction devices during transport; intermittent disconnection of suction from the gastric tube allows the pressures to equalize and prevents extreme suction against the gastric wall.
Children with a potential esophageal obstruction may benefit from an accompanying parent or other caregiver to decrease anxiety and prevent crying or other movement that may increase the risk of airway compromise.
Esophageal Varices
The most common cause of esophageal varices is hepatic congestion. Torturous, fragile, dilated esophageal veins can bleed from spontaneous rupture caused by increased portal hypertension or physical or chemical trauma. Esophageal varices are usually associated with cirrhosis. Varices occur frequently at the distal esophagus and hemorrhoidal plexus, and hemorrhagic shock from an esophageal bleed can occur rapidly. Bleeding occurs in 30% to 40% of patients who have esophageal varices. 10
Assessment
Sequential history of the patient with esophageal varices helps the transport team anticipate probable needs during transport.
Subjective Data
The transport team should obtain a history related to the cause of the esophageal varices, which can also provide information about other potential problems that could develop during transport. For example, the patient with severe liver disease also has bleeding and clotting problems. A patient with a history of alcoholism may be at risk for withdrawal, which may include seizures.
Objective Data
Careful consideration of the patient’s most recent pretransport laboratory data (hematocrit and hemoglobin levels, prothrombin time [PT]/partial thromboplastin time [PTT] or international normalized ratio [INR], and electrolyte profile) helps the transport team anticipate the patient’s needs during transport.
If transport is between medical facilities, a transport team member should review radiologic findings and ensure that adequate interventions have occurred. If a patient has undergone angiography, the transport team must secure the cannulization site before any patient movement and monitor the site frequently throughout transport.
Plan and Implementation
The transport team’s primary priority is to ensure adequacy of the airway before transport. The transport team must consider what supplies are needed should an acute hemorrhagic episode occur during transport. Continuous gastric suction can produce large volumes of secretions, and a system to adequately dispose of secretions during transport needs to be ready, such as a supply of sealable bags or containers with tight seals.
An experienced transport member must maintain adequate care of any esophageal tubes, such as the Sengstaken-Blakemore, Linton, or Minnesota tubes. Although these devices are rarely used anymore, traction-dependent or specialized esophageal tubes can pose a problem for transport. Traction maintained with a football helmet can be used during transport (Figure 25-1). A plan of care must be predetermined in the event of airway loss. 5
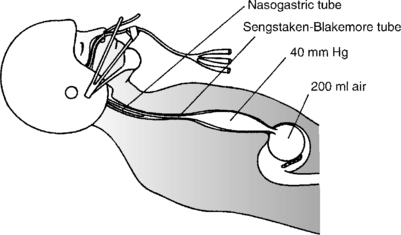 |
| FIGURE 25-1 Traction maintained with football helmet for Sengstaken-Blakemore tube. |
Airway loss from these particular types of tubes can be from either physiologic deterioration or tracheal obstruction. Saline solution, rather than air, can be used to inflate these cuffs to prevent further expansion during flight.
Intervention
If an acute hemorrhagic episode occurs, maintenance of airway and circulating volume is the first priority. Blood and blood product may be needed during transport. Effective pretransport planning to prevent vomiting and ensure adequate venous access and volume resuscitation is crucial. Management of medications such as vasopressin and octreotide is necessary during transport.
Because these patients may have active bleeding during transport, the transport team should prepare with additional suction equipment, suction catheters, and bedding. “Preplanning” is a good idea; perhaps the patient can be placed in a transport bag to prevent leakage of blood or fluids.
Esophageal Rupture
Esophageal rupture commonly results from penetrating trauma but may also result from a blunt insult to the thorax. Rupture from invading lesions, tumors, or caustic exposure also occurs but to a lesser extent. If esophageal rupture has occurred, the venting properties and pathways have been altered. During transport, and with possible altitude changes, the distribution and displacement of gases are no longer circumvented by the appropriate course. Complications of gastric pneumonitis, hemopneumothorax, and alteration in gas exchange may all occur.
Assessment
The transport team ascertains the history of incidents that led to the current episode. Drugs known to have corrosive effects on the esophagus are doxycycline, tetracycline, acetylsalicylic acid, clindamycin, potassium chloride, quinidine, and ferrous sulfate. Caustic substances can quickly lead to burning or complete erosion of the tissue. Estimation of the degree and size of burns is extremely difficult and can quickly compromise respiratory status. If the rupture is caused by an extravasating tumor, hemorrhage and airway control can become quite difficult.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:


Full access? Get Clinical Tree
