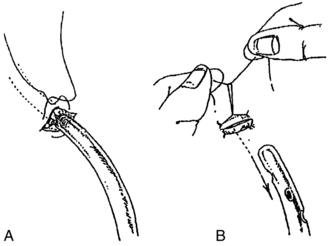
PROCEDURE 22 • Chest tubes are placed in the pleural or mediastinal space to evacuate an abnormal collection of air or fluid or both. • Indications for removal are based on the reason for insertion and include the following: • Air leaks have resolved for at least 24 hours (the absence of continuous bubbling in the water-seal chamber or absence of air bubbles from right to left in the air leak detector), and lung is fully reinflated on chest radiographic results. • The air leak detector should bubble gently immediately on insertion of the chest tube during expiration and with coughing. Continuous bubbling in the air leak detector indicates a leak in the patient or the chest drainage system. Fluctuations in the water level (also known as tidaling) in the water-seal chamber of 5 to 10 cm, rising during inhalation and falling during expiration, should be observed with spontaneous respirations. If the patient is on mechanical ventilation, the pattern of fluctuation is just the opposite. Any suction applied must be disconnected temporarily to assess correctly for fluctuations in the water-seal chamber. • Pleural tubes are placed after cardiac surgery if the pleural cavity has been entered. They typically are removed within 24 to 48 hours after surgery.1,9 • Mediastinal chest tubes most often are removed 24 to 36 hours after cardiac surgery.1 • Flexible Silastic (Blake) (Ethicon, Inc, Somerville, NJ) drains may be used in place of large-bore chest tubes in the mediastinal and pleural spaces after cardiac surgery. These tubes provide more efficient drainage and improved patient mobility with minimized tissue trauma and pain with removal.3,7,17 Pleural tubes placed for reasons other than postcardiac surgery necessity remain until the patient no longer needs them (i.e., no persistent air leak, stoppage of ongoing fluid leak or bleeding, or reexpansion of lung on chest radiograph). • Chest radiographs are done periodically to determine whether the lung has reexpanded. Daily chest radiographs are not necessary while the tube is in place.10 Reexpanded lungs, along with respiratory assessments that show improvement in the patient’s respiratory status, are the basis for the decision to remove the chest tube. • While the tubes are in place, patients may have related discomfort. Prompt removal of chest tubes encourages patients to increase ambulation and respiratory measures to improve lung expansion after surgery (e.g., coughing, deep breathing). However, removal of the chest tube may also be a painful procedure for the patient.4,8,15,16 • The types of sutures used to secure chest tubes vary according to the preference of the physician, the physician assistant, or the advanced practice nurse. One common type is the horizontal mattress or purse-string suture, which is threaded around and through the wound edges in a U-shape with the ends left unknotted until the chest tube is removed. Usually, one or two anchor stitches accompany the purse-string suture (Fig. 22-1). • A primary goal of chest tube removal is removal of tubes without introduction of air or contaminants into the pleural space. • Antiseptic swabs (povidone-iodine, chlorhexidine gluconate with alcohol, etc)6 • Petrolatum gauze, as per hospital protocol • Rubber-tipped Kelly clamps (two per chest tube) or disposable umbilical clamps • Wide occlusive tape (2-inch) • Elastic closure device, such as Steri-Strips (3M, St. Paul, MN) • Dry 4 × 4 gauze sponges (two to four)
![]() Chest Tube Removal (Perform)
Chest Tube Removal (Perform)
PREREQUISITE NURSING KNOWLEDGE
 Drainage has decreased to 50 to 200 mL in prior 24 hours if tube was placed for hemothorax, empyema, or pleural effusion.
Drainage has decreased to 50 to 200 mL in prior 24 hours if tube was placed for hemothorax, empyema, or pleural effusion.
 Research has shown that, depending on the reason for the chest tube, volumes of 200 to 450 mL/day do not adversely affect length of stay or overall costs when compared with lower threshold volumes, nor does the risk of pleural fluid reaccumulation increase.5,21
Research has shown that, depending on the reason for the chest tube, volumes of 200 to 450 mL/day do not adversely affect length of stay or overall costs when compared with lower threshold volumes, nor does the risk of pleural fluid reaccumulation increase.5,21
 Drainage has changed from bloody to serosanguineous, no air leak is present, and amount is less than 100 mL in the past 8 hours (if tube was placed after cardiac surgery).1,9
Drainage has changed from bloody to serosanguineous, no air leak is present, and amount is less than 100 mL in the past 8 hours (if tube was placed after cardiac surgery).1,9
 Lungs are reexpanded (as shown on chest radiographic results).
Lungs are reexpanded (as shown on chest radiographic results).
EQUIPMENT
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter

Full access? Get Clinical Tree


22: Chest Tube Removal (Perform)