Edited by George Jelinek George Jelinek and Sylvia Andrew-Starkey Essentials 1 Prevalence of mental health disorders appears to be increasing in Western society. 2 Regardless of diagnosis and presentation, three brief risk assessments must be performed within the first few minutes of an individual’s arrival in the emergency department (ED). These are: 3 The role of organic illness presenting as a behavioural disorder should not be forgotten. Mental health disorders are one of the three leading causes of total burden of disease and injury in Australia, alongside cancer and cardiovascular disease [1–3]. In middle age, it is the leading cause of non-fatal disease burden in the Australian population. There is no doubt that mental health disorders have a high prevalence, are disabling and are high cost in both human and socioeconomic terms [1,2]. In terms of disability, it has been estimated that having moderate to severe depression is the equivalent of having congestive cardiac failure [3], chronic severe asthma or chronic hepatitis B [2]. Severe post-traumatic stress syndrome was comparable to the disability from paraplegia and severe schizophrenia was comparable to quadriplegia, in terms of disability [2]. Over the 10 years to 2007, emergency department (ED) presentations rose 8% in the USA, whereas mental health presentations for the same time period rose 38%, contributing significantly to ED overcrowding [4]. This trend has been mirrored in Australia. The Australian Institute of Health and Welfare report into Mental Health Services in 2012 estimated that there were nearly a quarter of a million occasions of service to Australian EDs in 2009/10 where the primary problem was thought to be due to a mental health disorder, with an average annual increase of 3.6% between 2005–06 and 2009–10 [1]. A little over 3% of Australian public hospital ED presentations are for mental health related problems, correlating well with other studies and US figures, which estimate 2–6% of emergency medicine presentations are primarily due to mental health disorders [4–7]. Two-thirds of these people are between the ages of 15 and 44 years (compared to 42% for the general population presenting to a suburban ED); 29% have anxiety and neurotic disorders, 21% mental and behavioural disorders due to psychoactive substance abuse, 19% mood disorders and 17% schizophrenia or delusional disorders [4]. This is a significant underestimate of the prevalence of mental health disease in the ED as many patients remain undiagnosed and many have active medical conditions and a mental health diagnosis may be secondary [6]. It is estimated that 17.7% of adult Australians admitted to hospital report a mental health issue in the previous 12 months. An estimated 0.4–0.7% of the adult population suffer from a psychotic episode in any 1 year [2]. Mental health issues are highly prevalent and relevant. The mainstreaming of mental health patients into general EDs has brought problems and anxieties for staff. Staff often feel a lack of confidence because they are dealing with a population of patients unfamiliar to them. They can also feel inadequate due to poor assessment skills [7,8]. Recent Australian studies have shown ED clinicians are most concerned about knowledge gaps in risk assessment, particularly related to self-harm, violence and aggression, and distinguishing psychiatric from physical illness [9]. ED clinicians routinely report the need for more education on mental health related presentations [10]. A high proportion of mental health patients have drug and alcohol intoxication. This confounds the evaluation and treatment, lengthens the stay of these patients within the ED and delays their disposition. Mental health patients can be assigned lower triage categories and longer waits to be seen by staff than mainstream patients and there is more variation in triage categorization for mental health patients [11]. They have a higher chance of leaving before assessment has begun or is complete and the overall increase in length of assessment time has the potential to increase violence in the ED [7,8]. With this in mind, there has been much work over the last 10 years on the assessment of mental health patients in a general ED. It is important for health professionals assessing the mentally ill to be aware of their own potential biases. An interviewer’s past history and personal beliefs can influence a mental state assessment and the interviewer should be aware of this. These beliefs may stem from past personal or professional experience (Table 20.1.1). A mental state examination (MSE) is analogous to the management of severe trauma. There is an initial risk assessment looking for immediately life-threatening risks to the patient or staff. The triage nurse and the treating doctor should then obtain a brief collateral history from the emergency services or carers and initial management is based on this assessment. Regardless of threat, all assessments should balance the safety of both patient and staff with privacy and dignity [7]. Assessment should be based on [12]: If the situation is relatively controlled, the formal mental health assessment should then take place. Further information is gathered from the community. A provisional assessment and management plan is developed in conjunction with the mental health team and appropriate disposition is arranged (Fig. 20.1.1). The Mental Health Triage Scale (Table 20.1.2) has been developed and modified to be included into the Australian Triage Scale (ATS) [7,13,14]. It is very broad and asks the triage nurse to make four assessments: risk of suicide/self-harm, risk of aggression/harm to others, risk of absconding and whether the patient is intoxicated. From this, the triage nurse determines the ATS and urgency of initial treatment. It is also helpful to determine if the patient is known to a mental health service. Table 20.1.2 The mental health triage scale Many centres have developed a triage risk assessment proforma. For ease of use, many of these have included ‘tick box’ areas. A compilation of multiple assessment tools used throughout Australia is shown in Tables 20.1.3–20.1.5[2,5,12–15]. Table 20.1.3 Brief screening suicide risk template Table 20.1.4 ☑ Alert on chart ☑ Previous history of violence/threatening behaviour: verbal or physical ☑ Aggressive behaviour/thoughts ☑ Homicidal ideation ☑ Use of weapons previously ☑ Access to weapons ☑ Intoxicated ☑ Middle-aged male Patients then stratified into high, medium or low risk Table 20.1.5 Mode of arrival ☑ Police ☑ Handcuffed ☑ Family/carer coercion ☑ Voluntary ☑ Past history of absconding behaviour ☑ Alert on chart ☑ Verbalizing intent to leave ☑ Lack of insight into illness ☑ Poor/non-compliance with medication Patients then stratified into high, medium or low risk It is recommended that any patient who scores ‘high risk’ in any one area or ‘medium risk’ in two areas is treated as a ‘high-risk’ patient. Ensuing management of ‘high-risk’ patients depends on: local protocols, levels and presence of security, police intervention, restraint and sedation guidelines and guidelines for the urgent assessment by ED and/or by mental health services. The aims of the formal mental health assessment are to determine the following: Only if all of the above are answered, can management and appropriate disposition be considered. The environment in which the mental state assessment is conducted is important. Behaviourally disturbed people tolerate noise poorly and have short concentration spans. The interview room should be quiet, private, make the patient feel safe and the interviewer should avoid all interruptions. These prerequisites are increasingly difficult to attain in current access-blocked environments. The interviewer should sit at the same level as the patient and impart empathy. The voice should be quiet and calming. The interviewer should use non-judgemental language and open-ended questions [13,16]. It is important that the interviewer also feels safe and secure. If any risk is felt, the interviewer should have security or police present in the room or just outside. Depending on state legislation and hospital policy, the interviewer may request to have the patient searched. The interviewer should also note the nearest duress alarm and may choose to wear a personal alarm. The interviewer should sit within easy access of an exit and should never be boxed into a corner. If an interviewer begins to feel uncomfortable, there is always the option of leaving and returning to complete the assessment at a later stage. All threats, attempts and gestures suggestive of violence should be treated seriously. The formal interview has become less diagnosis focused and more problem based. Management is centred around the alleviation of symptoms and return to function. Thus, the psychiatric interview has become somewhat less structured. It is wise to establish rapport with the patient by personal introduction and explaining the purpose of the interview. The interviewer can begin by asking a series of non-threatening questions, such as demographics. This information is often required as many mental health services rely on an appropriate post code to determine follow-up management. These questions assist by building a profile of lifestyle, relationships and thought processes. Likelihood of success or failure of particular treatment modalities may be assisted by knowledge of previous hospital admissions, both general hospital and mental health (Table 20.1.6). Table 20.1.6 Demographic information required The process of obtaining a mental health assessment is different to that of a general medical assessment. In a general medical history, a series of questions is asked and the response is written. In a mental health assessment, responses are also interpreted. The interviewer is asked to form an opinion as to how thoughts are processed, based on observations. The interviewer is asked to interpret the patient’s thought patterns by what, and how, the patient tells the interviewer. The patient is asked to recall the sequence of events prior to presentation to the ED. The interviewer should explore the circumstances of the behaviour, reasons for it, degree of planning or impulsivity and its context. Were drugs and alcohol involved? Was there a recent precipitating event? It is often useful to get the patient to recall the previous 48–72 hours leading up to the event. This usually leads to questioning regarding current difficulties. The interviewer should explore the nature of current problems. They may be financial or legal problems, isolation, bereavement, impending or actual loss, or diagnosis of major illness. Have there been any recent changes and who are their usual support people? An exploration of significant relationships is important along with the depth and duration of these relationships. It is useful to explore the patient’s usual coping methods when under stress. There should be formal questioning regarding the patient’s mood (internal feelings) and whether it is in keeping with affect (external expression). The mood may be incongruent with affect, swing wildly between extremes (labile) or be inappropriate. Usually mood is assessed by asking about the patient’s ability to cope with activities of daily living, such as eating, weight loss or gain, sleep disturbance (early morning wakening or trouble getting to sleep) and general hygiene. The patient’s ability to concentrate may also diminish with increasing mood disturbance, reflected by the ability to perform normal work duties. This may lead to direct questioning regarding mood and thoughts of suicide. It is important to be direct in asking the patient about suicide and whether there is a formulated plan. A well thought out plan with clear means of carrying out threats is of great concern. Delusions and hallucinations are often personal and the patient may not want to disclose intimate thoughts and beliefs to the interviewer. Hallucinations may be auditory, visual, tactile, olfactory, somatic or gustatory. The context in which they occur should be explored. Hypnagogic (occurring just before sleep) and hypnopompic (occurring on wakening) hallucinations are more benign than others. Common themes for all types of hallucinations include suicide, persecution, religion, control, reference, grandeur or somatization. Insight is the degree of understanding of what is happening and why. This may be: It is important to determine the patient’s level of insight. This determines appropriate treatment and management, level of supervision required and the likelihood of compliance with treatment. The second part of the MSE can be more difficult to conceptualize. It relies on the interviewer actively observing the patient’s behaviour and conversation and interpreting thoughts. A summary is given in Table 20.1.7. Table 20.1.7 Overview of mental state examination This part of the interview can be difficult to remember and different services have developed a multitude of acronyms for remembering the various elements of the remaining mental health assessment. Listed below are two. ABC of Mental Health Assessment [12]: GFCMA – ‘Got Four Clients on Monday Afternoon’ [13]: This determines the patient’s ability to self-care. Table 20.1.8 lists features that may require particular attention. Attitude is important as it may indicate whether a patient is compliant with management and treatment. Abnormal posturing or repetitive behaviours should be noted. These may indicate increasing thought disturbance. With increasing aggression and agitation, there may be motor restlessness, pacing and hand wringing. Tension may escalate rapidly and steps should be taken early to diffuse the situation. Table 20.1.8 Appearance, attitude and behaviour The interviewer should note the rate, volume and rhythmicity of speech. This can range from completely mute, through monosyllabic answers, to rapid, loud speech indicative of pressure of speech. The tone, inflection, content and structure of speech should be noted. The interviewer should determine if the speech is fluent, if the thoughts behind it are logical and whether it flows appropriately for the situation. This is speech that does not reach its goal, is not fluent and is interrupted often with many pauses or changes in direction. A list with explanations is given in Table 20.1.9. Table 20.1.9 There are often recurrent themes in the speech of an acutely disturbed patient. These may revolve around suicide, persecution, control, reference, religion or somaticism (the extremes of which are nihilistic delusions – the belief that part of the self does not exist, is dead or decaying) or they may be grandiose in nature. A patient may be actively hallucinating despite denying this on questioning. It is important to note if the patient’s eyes suddenly switch direction for no apparent reason or they appear to be listening to a voice. These movements are often quite subtle and easily missed if observation is not active. A formal examination of cognitive function and a thorough physical examination complete the full psychiatric assessment. The interviewer should ensure that the patient does not have an acute confusional state secondary to a physical condition that may account for a behavioural problem. A number of tools are available to assess cognitive functioning. These comprise assessments in orientation, concentration, memory, language, abstraction and judgement. An assessment of a patient’s cognitive functioning and intelligence may assist in deciding the best way to deal with problems. Approximately 20% of mental health patients have a concurrent active medical disorder requiring treatment and possibly contributing to the acute behavioural disturbance [6]. Investigations depend on physical findings but may include creatine kinase, urine drug screen, electroencephalogram, computed tomography and lumbar puncture. Only after this can an emergency medicine practitioner plan the most appropriate management. Although time consuming, a good mental health assessment is vital for the appropriate management and disposition of what is an increasingly large group of patients in the ED. If able to formulate an opinion on the risk assessments regarding suicide, violence and flight risk and the aims of the MSE, the emergency clinician will be able to present to mental health services a comprehensive picture of the patient. The mental health professional is then able to administer mental health first aid [2], the principles of which are:
Psychiatric Emergencies
20.1 Mental state assessment
Epidemiology
Introduction to the mental state examination
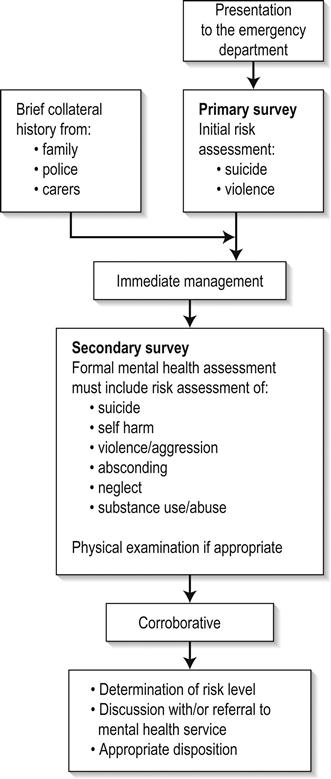
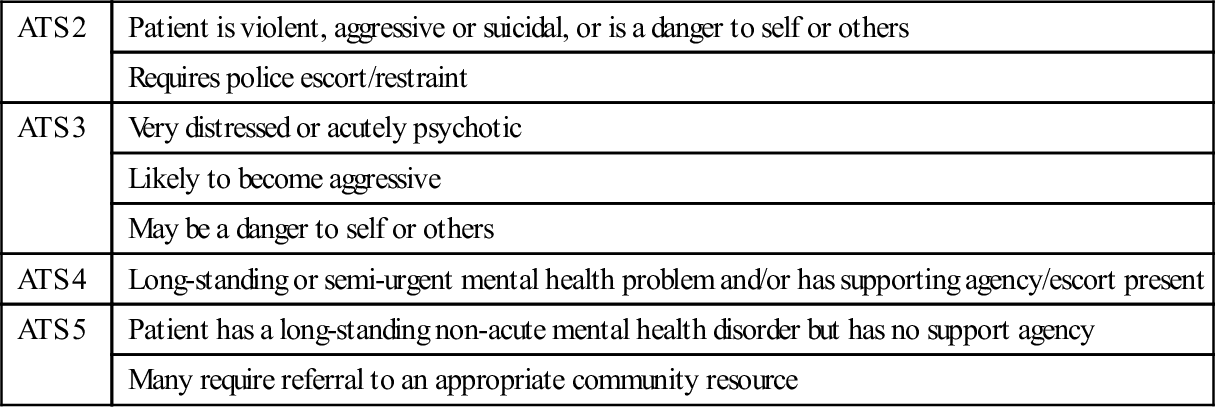
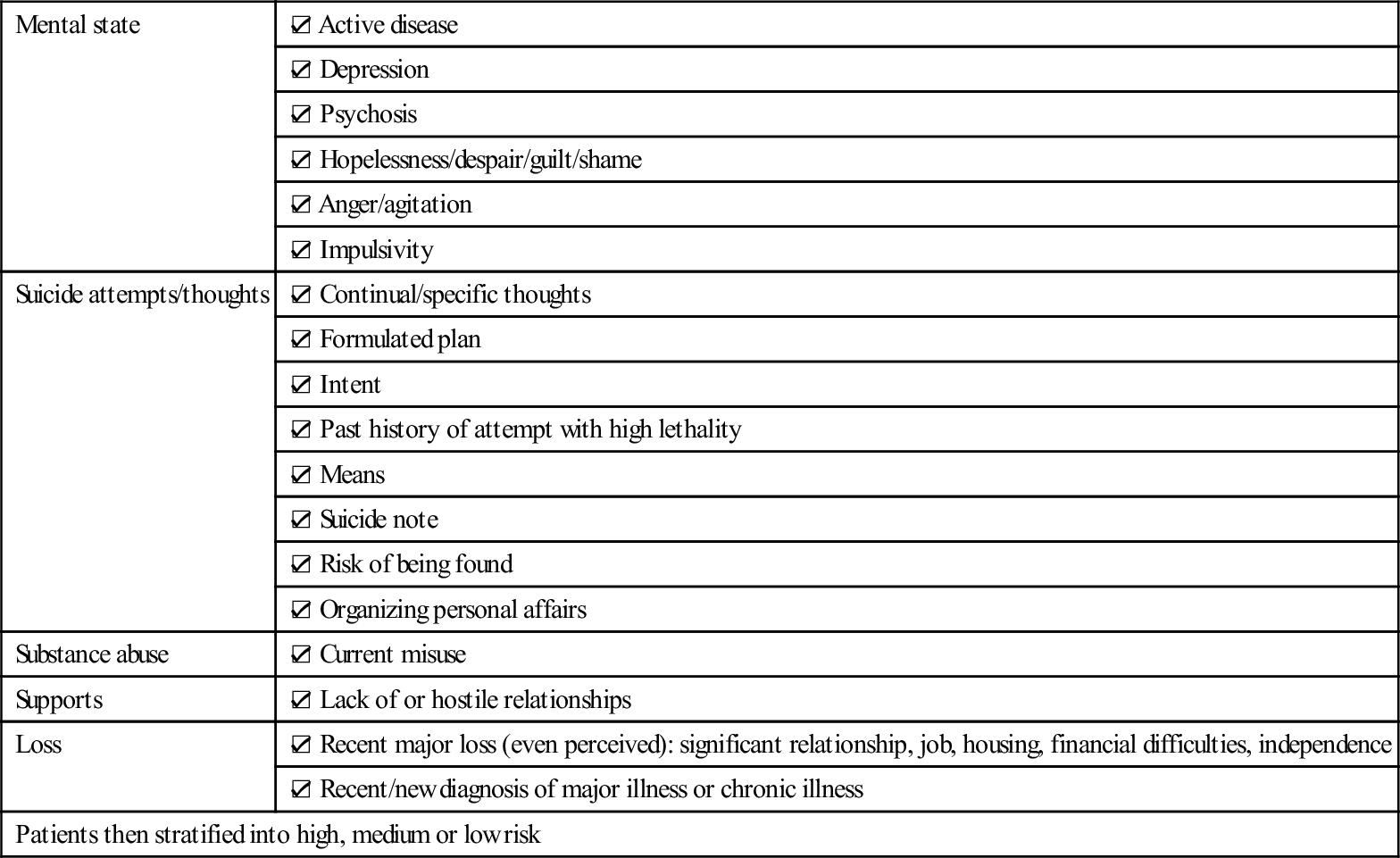
Bias and discrimination
ABC of the MSE
Triage
ATS 2
Patient is violent, aggressive or suicidal, or is a danger to self or others
Requires police escort/restraint
ATS 3
Very distressed or acutely psychotic
Likely to become aggressive
May be a danger to self or others
ATS 4
Long-standing or semi-urgent mental health problem and/or has supporting agency/escort present
ATS 5
Patient has a long-standing non-acute mental health disorder but has no support agency
Many require referral to an appropriate community resource
Mental state
☑ Active disease
☑ Depression
☑ Psychosis
☑ Hopelessness/despair/guilt/shame
☑ Anger/agitation
☑ Impulsivity
Suicide attempts/thoughts
☑ Continual/specific thoughts
☑ Formulated plan
☑ Intent
☑ Past history of attempt with high lethality
☑ Means
☑ Suicide note
☑ Risk of being found
☑ Organizing personal affairs
Substance abuse
☑ Current misuse
Supports
☑ Lack of or hostile relationships
Loss
☑ Recent major loss (even perceived): significant relationship, job, housing, financial difficulties, independence
☑ Recent/new diagnosis of major illness or chronic illness
Patients then stratified into high, medium or low risk
Aims of mental health assessment
 Does the patient have a mental illness?
Does the patient have a mental illness?
 Is there a question of safety for the patient or for others?
Is there a question of safety for the patient or for others?
 Does the patient have insight into the illness?
Does the patient have insight into the illness?
 Will the patient comply with suggested treatment?
Will the patient comply with suggested treatment?
 Can the patient be managed in the community or is hospitalization required?
Can the patient be managed in the community or is hospitalization required?
The formal psychiatric interview
Introduction
First part of the interview: direct questioning
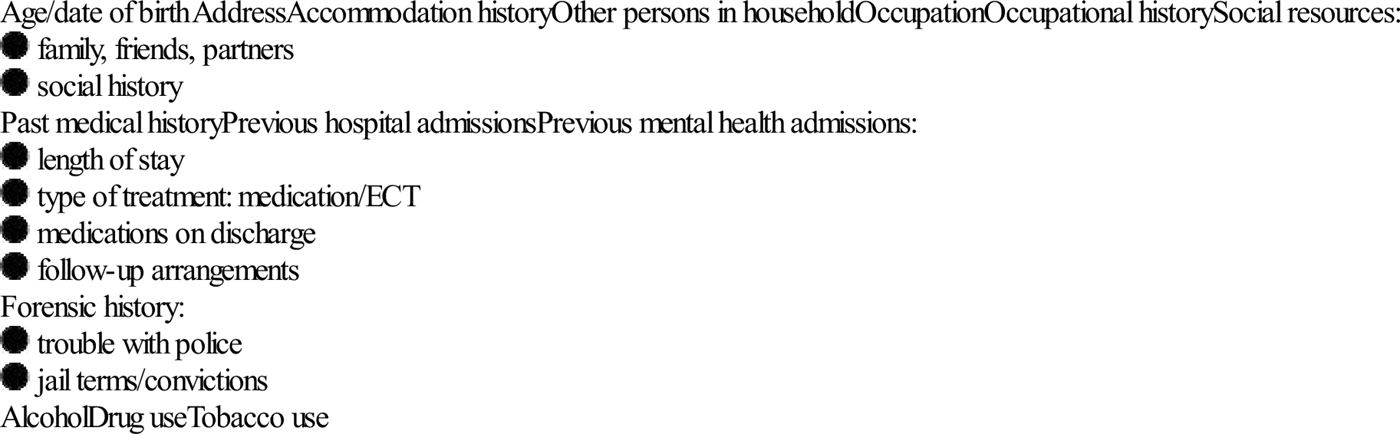
Basic demographic information
Presenting complaint
Mood and affect
Delusions and hallucinations
Insight and judgement
 awareness of being sick and needing help but denying it at the same time
awareness of being sick and needing help but denying it at the same time
 awareness of being sick but blaming it on external factors
awareness of being sick but blaming it on external factors
 awareness that illness is due to something unknown within the patient
awareness that illness is due to something unknown within the patient
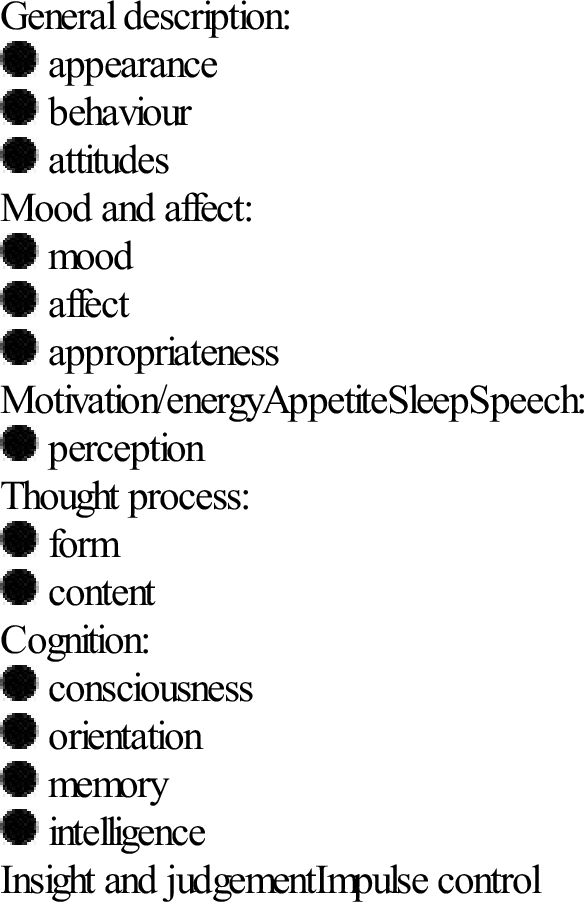
Second part of interview: observation
Key elements
General description:
Mood and affect:
Motivation/energy
Appetite
Sleep
Speech:
Thought process:
Cognition:
Insight and judgement
Impulse control
Appearance, attitude and behaviour
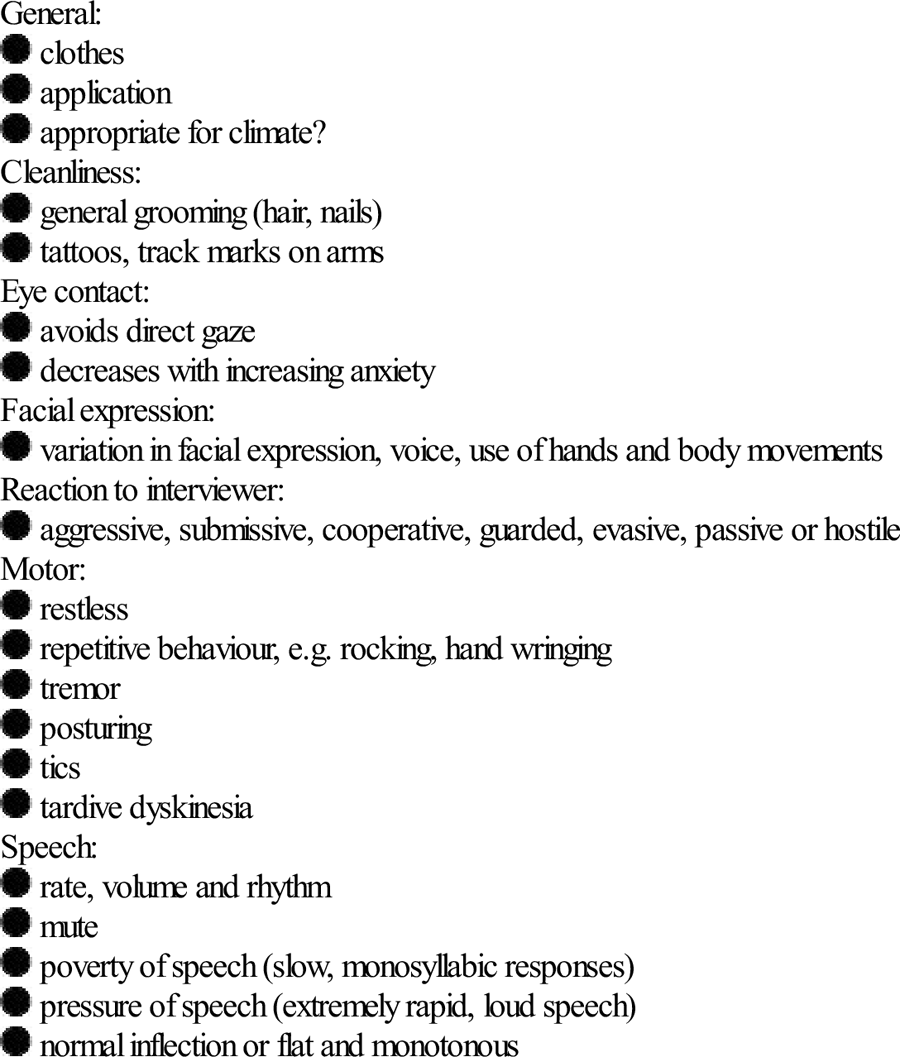
Thought disorder
Circumstantiality
Delays in reaching goals by long-winded explanations, but eventually gets there
Distractible speech
Changes topic according to what is happening around the patient
Loosening of associations
Logical thought progression does not occur and ideas shift from one subject to another with little or no association between them
Flight of ideas
Fragmented, rapid thoughts that the patient cannot express fully as they are occurring at such a rapid rate
Tangentiality
Responses that superficially appear appropriate, but which are completely irrelevant or oblique
Clanging
Speech where words are chosen because they rhyme and do not make sense
Neologisms
Creation of new words with no meaning except to the patient
Thought blocking
Interruption to thought process where thoughts are absent for a few seconds and are unable to be retrieved
Thought content
Perception
Cognitive assessment and physical examination
Conclusion
 assess the risk of suicide/harm to others
assess the risk of suicide/harm to others
 give reassurance and information
give reassurance and information
 encourage getting professional help
encourage getting professional help

Full access? Get Clinical Tree


20. Psychiatric Emergencies