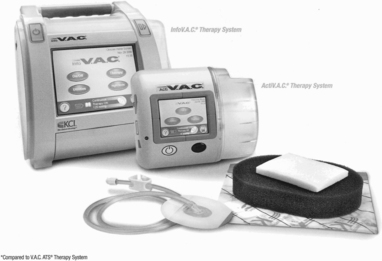
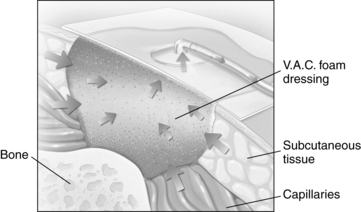
PROCEDURE 131 • Negative-pressure wound therapy (NPWT) is an advanced wound care therapy that uses an occlusive wound dressing, tubing, and powered vacuum unit with a collection canister. Other terms found in the literature for NPWT include topical negative therapy (TPN) and subatmospheric pressure therapy. • Many different U.S. Food and Drug Administration (FDA)–approved vacuum units are on the market for NPWT.10 The Agency for Healthcare Research and Quality (AHRQ) provides a review of current NPWT manufacturers.11 The most common devices seen in the acute care practice setting are ActiV.A.C.® and InfoV.A.C. Therapy Systems (KCI Licensing, Inc., San Antonio, TX; Fig. 131-1) and RENASYS EZ® (Smith & Nephew, St. Petersburg, FL8; Fig. 131-2). ActiV.A.C.® and Info V.A.C.®12 use a patented open-cell foam wound contact dressing, and RENASYS EZ®6 (and other newly developing units on the market) uses either an open-cell foam or the vacuum-pack method with an antimicrobial gauze packing dressing. The use of moistened gauze wound interface has also been reported in the literature as an effective dressing for NPWT.7 • Most randomized controlled studies and case studies on NPWT have been conducted with the V.A.C. therapy. No randomized controlled trials are found that compare the effectiveness of various NPWT techniques or systems.11 Further clinical research to evaluate wound closure outcomes with the different NPWT units is needed.5,8,10,11 • NPWT assists with wound closure by applying a controlled subatmospheric (negative) pressure evenly over a wound bed. This mechanical stress creates a noncompressive force on the wound bed that dilates the arterioles, increasing the effectiveness of local circulation and enhancing the proliferation of granulation tissue.1,4,5 NPWT enhances lymphatic flow and removal of excessive fluid, decreasing wound edema and bacterial load at the wound site, further aiding wound healing (Fig. 131-3).1,2,4,5,9,10 • Wound healing is best achieved through adequate cleansing, débridement, and dressing of the wound bed on the basis of patient and wound characteristics. • Wounds heal by either primary or secondary intention (see Fig. 126-1). Most clean surgical wounds heal by primary intention. Suturing each layer of tissue approximates the wound edges. These wounds typically heal quickly and require minimal wound care. Contaminated surgical or traumatic wounds (open wounds) heal by secondary intention. Wounds that heal by secondary intention granulate from the base of the wound to the skin surfaces; care must be taken to allow for uniform granulation and prevention of open pockets or tunneling. • Openly granulating wounds heal more slowly and must remain moist to enhance tissue granulation. Wound care for these wounds focuses on maintaining a moist environment free of necrotic tissue, and decreasing pain. • Open wounds may have excessive wound drainage that necessitates application of absorptive dressings, protection of periwound skin, and more frequent dressing changes to facilitate healing. NPWT provides wound drainage management and decreased frequency of dressing changes (most NPWT dressing changes are three times per week) with improved pain management. • NPWT has been approved by the U.S. FDA for the following wounds: • Goals of NPWT in the management of wounds may include wound bed preparation for skin grafts, full wound closure, decrease in wound size, removal of wound edema for delayed primary closure, and increased perfusion to marginally viable flaps. • The effectiveness of NPWT should be evaluated with each dressing change to include a comprehensive wound assessment and weekly wound measurements. If wound measurements have not improved at least 15% after 2 weeks of therapy, reevaluate the continuation of NPWT with reassessment of wound healing variables.13 • Wounds with infections should have systemic antibiotic treatment before initiation of NPWT. If continued deterioration of the wound or infection persists, consider discontinuation of NPWT with possible evaluation for surgical drainage of infection per healthcare provider. • Wounds treated with NPWT develop a characteristic, beefy red granulation bed. Pale, friable granulation tissue is a secondary sign of infection and may be more reliable than the traditional indicators of infection.3 • Dehisced infected sternal wounds with use of NPWT require effective débridement of infected bone and a specific nonadherent wound contact layer before a NPWT dressing is placed. • Successful management of enteric fistulae with NPWT with use of special application techniques has been reported in case studies but no clinical trials at this time. See NPWT device manuals for specific techniques in the management of fistulae.
Negative-Pressure Wound Therapy
PREREQUISITE NURSING KNOWLEDGE
 Acute wounds (orthopedic trauma wounds, partial-thickness burns, abdominal wounds, surgical dehisced wounds, flaps, and grafts)
Acute wounds (orthopedic trauma wounds, partial-thickness burns, abdominal wounds, surgical dehisced wounds, flaps, and grafts)
 Chronic wounds (diabetic wounds, pressure ulcers, leg ulcers)
Chronic wounds (diabetic wounds, pressure ulcers, leg ulcers)
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 20: Chest Tube Placement (Perform)
20: Chest Tube Placement (Perform)
![]() 95: Lumbar Puncture (Perform)
95: Lumbar Puncture (Perform)
![]() 35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes
35: Invasive Mechanical Ventilation (Through an Artificial Airway): Volume and Pressure Modes

Full access? Get Clinical Tree


131: Negative-Pressure Wound Therapy