PROCEDURE 116 • Therapeutic apheresis (i.e., hemapheresis) is a technique for selective removal of cells, plasma, and substances from the patient’s circulation to promote clinical improvement. The different apheresis techniques vary according to the component of the blood removed or replaced or the substance removed. • During plasma exchange procedures, the plasma removed must be replaced; the most common replacement fluids are albumin, fresh frozen plasma (FFP), thawed plasma (derived from thawed FFP and maintained at low temperatures for use within 1 to 5 days), and normal saline.1 Because clotting factors are transiently reduced by plasma exchange, FFP can also be used as a fluid replacement in patients when bleeding is an issue. • Plasma volume is an estimate of the patient’s total volume based on gender, height, weight, and hematocrit value. Exchange volume is the ratio of the patient’s plasma volume to be removed and replaced; this is usually 1:1 or 1.5:1 of the patient’s estimated plasma volume.4 • In plasma exchange, an average of 3 to 5 L of plasma is removed and replaced.4 • Treatments can be done with two different machines.4 • Treatment length and frequency vary according to the disease being treated, rate of production of the substance being removed, and the patient’s response to treatment. Acute conditions, such as thrombotic thrombocytopenia purpura or graft-versus-host disease, usually require daily treatments for 5 to 7 days.6,7 Other conditions usually require plasma exchanges two or three times weekly for up to 6 weeks.2,5–7 The total amount of plasma to be exchanged is used as a guide for treatment. A single treatment, referred to as a plasma exchange, usually takes 2 to 3 hours with a centrifugal machine and 2 to 6 hours with filtration methods.4 • Apheresis procedures are performed by healthcare professionals such as registered nurses or blood bank personnel, with special knowledge and skills in apheresis. These procedures are commonly performed both in critical care units and on an outpatient basis, depending on the type of disease being treated and on the patient’s condition. • The most commonly used apheresis systems use two large-bore peripheral venous catheters, a double-lumen vascular access catheter (VAC), or a dialysis graft or fistula to access the vascular system. Peripherally inserted central venous catheters or implantable venous access ports do not provide for adequate blood flow and are not acceptable for use.4 • The system should be primed with an anticoagulant (e.g., heparin or citrate) to prevent clotting. If citrate is used, the patient must be monitored closely for hypocalcemia. Citrate works as an anticoagulant by binding calcium (Ca++), therefore decreasing the amount of Ca++ available for normal clotting.4 • Plasma exchange is used to treat antibody-mediated disorders because the pathogenic antibodies are contained in the plasma. Removal of these antibodies through plasma exchange reduces the number of circulating antibodies, temporarily decreasing the patient’s symptoms.
Apheresis and Therapeutic Plasma Exchange (Assist)
PREREQUISITE NURSING KNOWLEDGE
 Plasma exchange is the process of replacing the plasma removed with an equal amount of either plasma or fluid (most commonly a combination of 5% albumin and normal saline solution).
Plasma exchange is the process of replacing the plasma removed with an equal amount of either plasma or fluid (most commonly a combination of 5% albumin and normal saline solution).
 Erythrocytapheresis is the process of removing erythrocytes (red blood cells) from whole blood.
Erythrocytapheresis is the process of removing erythrocytes (red blood cells) from whole blood.
 Thrombocytapheresis is the selective removal of platelets (thrombocytes).
Thrombocytapheresis is the selective removal of platelets (thrombocytes).
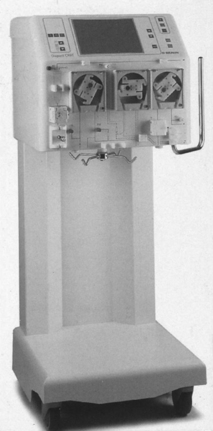
 Centrifugal apheresis machine: Separates plasma and other blood components with use of a centrifuge (Fig. 116-1).
Centrifugal apheresis machine: Separates plasma and other blood components with use of a centrifuge (Fig. 116-1).
 Filtration: A hollow-fiber cell separator, permeable to plasma proteins, is used to remove the patient’s plasma via an apheresis machine or continuous renal replacement machines adapted for pheresis (Fig. 116-2).
Filtration: A hollow-fiber cell separator, permeable to plasma proteins, is used to remove the patient’s plasma via an apheresis machine or continuous renal replacement machines adapted for pheresis (Fig. 116-2).
Related posts:
![]() 39: Automated External Defibrillation
39: Automated External Defibrillation
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter

Full access? Get Clinical Tree


116: Apheresis and Therapeutic Plasma Exchange (Assist)