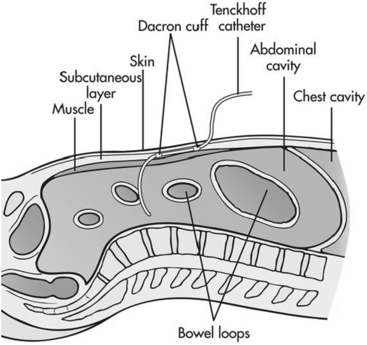
PROCEDURE 114 • Peritoneal dialysis (PD) works on the principles of diffusion and osmosis; thus, a basic knowledge of these concepts is necessary. • PD uses the peritoneal membrane as the semipermeable membrane for both fluid and solutes.4,10,14 • Sterile dialysis fluid (dialysate) is infused into the peritoneal cavity of the abdomen through a flexible catheter (Fig. 114-1). • A small-framed adult can usually tolerate 2 to 2.5 L of dialysate, whereas a large-framed adult may be able to tolerate up to 3 L in the abdominal cavity. The larger the volume of dialysate, the more effective the removal of blood urea nitrogen (BUN) and creatinine6,9,11; however, peritoneal clearance may be improved with more frequent exchange rather than an increase in the exchange volume.5 The most limiting factor of the volume of dialysate is that it may cause direct pressure on the diaphragm and cause a compromise of respiratory excursion.4,14,15 The PD dialysate contains higher concentrations of glucose than normal serum levels. These higher concentrations aid in the removal of water via osmosis and small-to-middle-weight molecules (urea, creatinine) via diffusion. Several concentrations of glucose are available in commercially prepared dialysate solutions. The higher the concentration of glucose in the dialysate, the greater the amount of fluid removal. Icodextrin, a relatively new alternative to glucose solutions, may be used as the osmotic agent. This glucose polymer is metabolized to maltose and is not readily absorbed.6,8,12,13 • PD involves repeated fluid exchanges or cycles. Each cycle has three phases: instillation, dwell, and drain. • PD can be performed either manually with a dialysis administration set with a drainage bag or with a cycler machine (Fig. 114-2). With a cycler machine, multiple exchanges are programmed into the machine and run automatically. Cycler machines are infrequently found in the hospital setting but are often used by outpatients for evening and night exchanges. • PD catheters can become clogged with the build-up of fibrin. Heparin is sometimes added to the dialysate or used as a separate flush to prevent occlusion.1,4,9,14,15 • PD dialysate should be warmed to the appropriate temperature in a commercial warmer. Never warm the solution in a standard microwave oven, which heats unevenly and does not regulate the fluid temperature.14,15 • After each cycle of PD, assess the patient’s vital signs, fluid balance, and any signs of infection and communicate abnormal findings to the physician. • The adequacy of dialysis and assessment of the patient’s residual renal function should be evaluated on a periodic basis. Adequacy of dialysis can be measured with urea kinetic modeling (Kt/V) or urea clearance.6,11
Peritoneal Dialysis
PREREQUISITE NURSING KNOWLEDGE
 Diffusion is the passive movement of solutes through a semipermeable membrane from an area of higher concentration to one of lower concentration. When this concept is applied to peritoneal dialysis, diffusion occurs because the patient’s blood contains waste products (solute), which give it a higher osmolarity (concentration) than the dialysate. So, waste products in the blood diffuse across the semipermeable membrane into the dialysate solution.
Diffusion is the passive movement of solutes through a semipermeable membrane from an area of higher concentration to one of lower concentration. When this concept is applied to peritoneal dialysis, diffusion occurs because the patient’s blood contains waste products (solute), which give it a higher osmolarity (concentration) than the dialysate. So, waste products in the blood diffuse across the semipermeable membrane into the dialysate solution.
 During the instillation phase, the dialysate is infused via gravity into the patient’s peritoneal cavity through a peritoneal catheter.1,2,12
During the instillation phase, the dialysate is infused via gravity into the patient’s peritoneal cavity through a peritoneal catheter.1,2,12
Related posts:
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]() 44: Emergent Open Sternotomy (Assist)
44: Emergent Open Sternotomy (Assist)

Full access? Get Clinical Tree


114: Peritoneal Dialysis