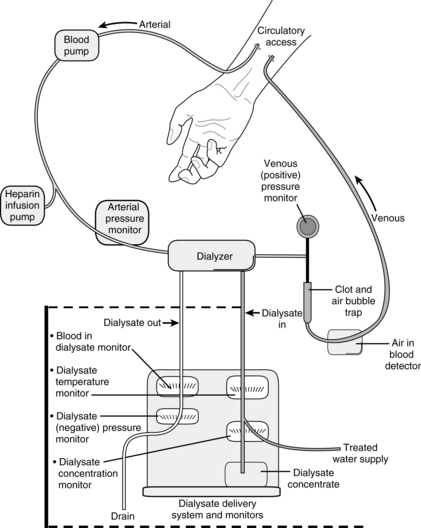
PROCEDURE 113 • Hemodialysis (Fig. 113-1) may be needed for the onset of acute renal failure, for maintenance therapy for patients with chronic renal failure, or for patients with acute drug intoxication.9 • Requirements for ensuring adequate therapy include: 1, an appropriate prescription; 2, a high level of nursing expertise; 3, an efficiently operating hemodialysis machine; 4, satisfactory access; 5, an informed patient; and 6, ongoing data review.11 • Knowledge of the principles of diffusion, ultrafiltration (UF), osmosis, oncotic pressure, and hydrostatic pressure as they pertain to fluid and solute management during dialysis is neccessary.2,4,5 • Vascular access is needed to perform hemodialysis and can be provided with a double-lumen vascular access catheter (VAC), an external arteriovenous (AV) shunt, or a surgically created AV anastomosis (e.g., fistula or graft). Common sites for the VAC include the internal jugular or subclavian vein. Common sites for the external shunt include the forearm (radial artery to cephalic vein) or the leg (posterior tibial artery to long saphenous vein). The AV fistula or graft is used for long-term dialysis management. • The subclavian vein is not recommended for temporary access because of the increased incidence of vascular stenosis, which makes the vein of the ipsilateral arm unsuitable for chronic dialysis if needed. The internal jugular or leg veins are more commonly used. • Hemodialysis uses an artificial kidney (hemofilter, dialyzer) with a semipermeable membrane to create two separate compartments: the blood compartment and the dialysis solution (dialysate) compartment. The semipermeable membrane allows the movement of small molecules (e.g., electrolytes, urea, drugs) and middle-weight molecules (creatinine) from the patient’s blood into the dialysate but is impermeable to larger molecules (blood cells, plasma proteins). • Each dialyzer has four ports: two end ports for blood (in one end and out the other) and two side ports for dialysis solution (also in one end and out the other). In most cases, the blood and dialysate are run through the dialyzer in opposite or countercurrent directions. • The hollow-fiber dialyzer is the most commonly used dialyzer. With this dialyzer, the blood flows through the center of hollow fibers and the dialysate flows around the outside of the hollow fibers. The advantages of hollow-fiber filters include a low priming volume, low resistance to flow, and high amount of surface area. The major disadvantage is the potential for clotting because of the small fiber size. • Parallel-plate dialyzers are designed as sheets of membrane over supporting structures. Blood and dialysate pass through alternate spaces of the dialyzer. The major disadvantages of this type of filter are the increase in allergic dialyzer reactions and lower filter surface area. • All dialyzers have UF coefficients; thus, the dialyzer selected varies in different clinical situations. The higher the UF coefficient, the more rapid the fluid removal. UF coefficients are determined with in vivo measurements done by each dialyzer manufacturer. • Clearance refers to the ability of the dialyzer to remove metabolic waste products from the patient’s blood. The blood flow rate, the dialysate flow rate, and the solute concentration affect clearance. Clearance occurs by the processes of diffusion, convection, and UF.2–4,8–10 • The blood circuit consists of blood lines, a blood pump, and various monitoring devices. The blood lines carry the blood to and from the patient. The blood pump controls the speed of the blood through the circuit. The monitoring devices include arterial and venous pressure monitors and an air detection monitor to prevent air entering the circuit from being returned to the patient. • The dialysate is composed of water, a buffer (e.g., acetate or bicarbonate), and various electrolytes. Most solutions also contain glucose. The buffer helps neutralize acids that are generated as a result of normal cellular metabolism and usually are excreted by the kidney. The concentration of electrolytes is usual normal plasma concentrations, which help to create a concentration gradient for removal of excess electrolytes. The glucose, available in various concentrations, promotes the removal of plasma water. • Heparin is usually used during dialysis to prevent clotting of the circuit. In patients with coagulopathies, normal saline solution flushes can be used to keep the blood circuit patent.5 Heparin should be avoided in patients with a history of heparin-induced thrombocytopenia (HIT).2,10 • Because large volumes of water are used during treatments to generate the dialysate, the water must be purified before patient use to prevent patient exposure to potentially harmful substances present in the water supply (e.g., calcium carbonate, sodium chloride, and iron). • Other extended renal replacement therapy techniques or “hybrid” techniques (sustained low-efficiency dialysis [SLED], extended daily dialysis [EDD]) generally use standard hemodialysis equipment and techniques with reduced blood flow and dialysate rates to gradually remove plasma water and solutes in the critically ill patient. They are used from 4 to 12 hours a day.8 • The adequacy of dialysis and assessment of the patient’s residual renal function should be evaluated on a periodic basis. Adequacy of dialysis can be measured with urea kinetic modeling (Kt/V) or urea clearance.2
Hemodialysis
PREREQUISITE NURSING KNOWLEDGE
 Diffusion is the passive movement of solutes through a semipermeable membrane from an area of higher to lower concentration until equilibrium is reached.
Diffusion is the passive movement of solutes through a semipermeable membrane from an area of higher to lower concentration until equilibrium is reached.
Related posts:
![]() 139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
139: Calculating Doses and Flow Rates and Administering Continuous Intravenous Infusions
![]() 16: Continuous Venous Oxygen Saturation Monitoring
16: Continuous Venous Oxygen Saturation Monitoring
![]() 132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
132: Small-Bore Feeding Tube Insertion Using an Electromagnetic Guidance System (CORTRAK®)
![]() 83: Implantable Venous Access Device: Access, Deaccess, and Care
83: Implantable Venous Access Device: Access, Deaccess, and Care
![]() 64: Blood Sampling from an Arterial Catheter
64: Blood Sampling from an Arterial Catheter
![]() 44: Emergent Open Sternotomy (Assist)
44: Emergent Open Sternotomy (Assist)

Full access? Get Clinical Tree


113: Hemodialysis